{"title":"Predicting the Need for Tertiary Trauma Care Using a Multivariable Model: A 4-Year Retrospective Cohort Study.","authors":"Piraya Vichiensanth, Kantawat Leepayakhun, Chaiyaporn Yuksen, Chetsadakon Jenpanitpong, Suteenun Seesuklom","doi":"10.22037/aaemj.v13i1.2581","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Delays in accessing an appropriate level of care can lead to significant morbidity or even mortality of trauma patients. This study aimed to develop a simplified prehospital predictive model to determine the need for tertiary care trauma centers (TTC), enabling timely and appropriate transport decisions by emergency medical service (EMS) teams.</p><p><strong>Methods: </strong>This is a retrospective cohort study conducted at the emergency department (ED) of Ramathibodi Hospital between January 2020 and April 2024. Prehospital trauma patients aged ≥15 years who were transported by EMS were included in the study. Patients were divided into two groups with and without the need for TTC, and the independent predictive factors of the need for TTC were explored using multivariable regression analysis.</p><p><strong>Results: </strong>The study included 440 trauma patients, with 31.1% requiring TTC. The predictors of the need for TTC included age (coefficient (Coef.) -0.003; 95% confidence interval (CI): -0.018 to 0.012; P=0.693), traffic mechanism (Coef. 0.848; 95%CI: 0.150 to 1.546; P=0.017), respiratory rate (Coef. 0.044; 95%CI: -0.037 to 1.124; P=0.285), heart rate (Coef. -0.004; 95%CI: -0.020 to 0.012; P=0.610), and Glasgow Coma Scale (Coef. -0.312; 95%CI: -0.451 to -0.173; P<0.001). The predictive model categorized patients into low, moderate, and high-risk groups. Patients who were categorized in the high-risk group showed a positive likelihood ratio (LHR+) of 14.88 for requiring TTC. The model achieved an area under the receiver operating characteristic curve (AuROC) of 73%, indicating the good discriminative ability of this prediction model.</p><p><strong>Conclusions: </strong>The predictive model classifies trauma patients into three risk groups based on five prognostic variables, which are able to predict the likelihood of requiring TTC. Internal validation has verified its high level of accuracy in trauma triage.</p>","PeriodicalId":8146,"journal":{"name":"Archives of Academic Emergency Medicine","volume":"13 1","pages":"e37"},"PeriodicalIF":2.0000,"publicationDate":"2025-03-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12065032/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of Academic Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22037/aaemj.v13i1.2581","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Delays in accessing an appropriate level of care can lead to significant morbidity or even mortality of trauma patients. This study aimed to develop a simplified prehospital predictive model to determine the need for tertiary care trauma centers (TTC), enabling timely and appropriate transport decisions by emergency medical service (EMS) teams.
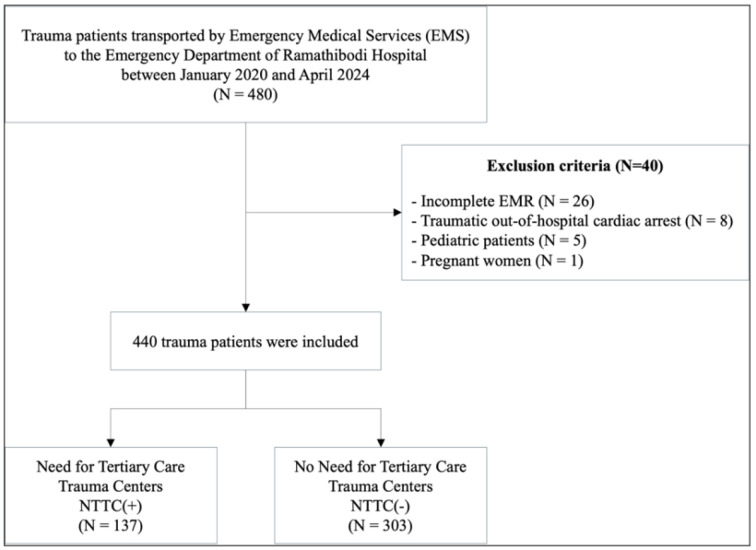
Methods: This is a retrospective cohort study conducted at the emergency department (ED) of Ramathibodi Hospital between January 2020 and April 2024. Prehospital trauma patients aged ≥15 years who were transported by EMS were included in the study. Patients were divided into two groups with and without the need for TTC, and the independent predictive factors of the need for TTC were explored using multivariable regression analysis.
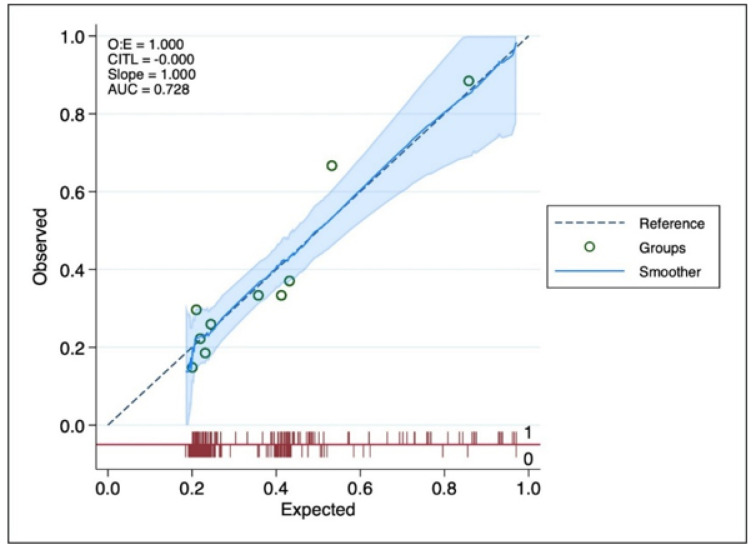
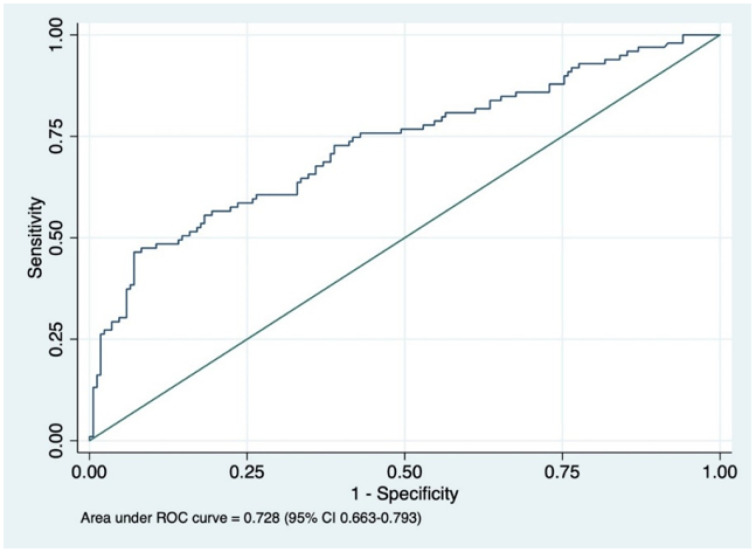
Results: The study included 440 trauma patients, with 31.1% requiring TTC. The predictors of the need for TTC included age (coefficient (Coef.) -0.003; 95% confidence interval (CI): -0.018 to 0.012; P=0.693), traffic mechanism (Coef. 0.848; 95%CI: 0.150 to 1.546; P=0.017), respiratory rate (Coef. 0.044; 95%CI: -0.037 to 1.124; P=0.285), heart rate (Coef. -0.004; 95%CI: -0.020 to 0.012; P=0.610), and Glasgow Coma Scale (Coef. -0.312; 95%CI: -0.451 to -0.173; P<0.001). The predictive model categorized patients into low, moderate, and high-risk groups. Patients who were categorized in the high-risk group showed a positive likelihood ratio (LHR+) of 14.88 for requiring TTC. The model achieved an area under the receiver operating characteristic curve (AuROC) of 73%, indicating the good discriminative ability of this prediction model.
Conclusions: The predictive model classifies trauma patients into three risk groups based on five prognostic variables, which are able to predict the likelihood of requiring TTC. Internal validation has verified its high level of accuracy in trauma triage.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


