{"title":"Association of Systemic Inflammatory Response Index with the cardiometabolic multimorbidity among US adults: A population-based study.","authors":"Jing Li, Songfeng Zhao, Xiaowen Zhang, Mengyan Fan, Jiaxin Wan, Rijin Lin, Feng Fan, Guo Liu, Sheng Guan, Aihua Liu","doi":"10.4103/bc.bc_32_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Chronic inflammation plays an essential role in the occurrence and progression of cardiometabolic diseases (CMDs). We aim to examine the association between a novel inflammatory biomarker Systemic Inflammatory Response Index (SIRI) and different cardiometabolic multimorbidity (CMM) statuses.</p><p><strong>Methods: </strong>This was a cross-sectional study that includes general participants of the National Health and Nutrition Examination Survey database from 1999 to 2018. SIRI was calculated as neutrophil count × lymphocyte count/monocyte count. The CMDs were defined as a series of diseases including diabetes mellitus (DM), heart disease (HD), and stroke. We explored the association of SIRI with outcomes with weighted multivariable logistic regression models weighted restricted cubic spline. The diagnostic value of SIRI was evaluated using weighted receiver operating characteristic (ROC) curves.</p><p><strong>Results: </strong>A total of 43,345 participants were enrolled with a mean age of 45.86 years. The weighted prevalence of CMD and CMM was 17.14% and 2.94%, respectively. Compared to those without CMD, the adjusted odds ratios (95% confidence interval) for each unit increase in SIRI were 1.14 (1.09-1.19) for DM, 1.13 (1.07-1.19) for HD, 1.11 (1.04-1.19) for stroke, 1.17 (1.12-1.22) for CMD, and 1.16 (1.10-1.23) for CMM, according to the weighted multivariable logistic regression. Elevated SIRI level was independently associated with increased CMM. There was no interaction found in subgroup analysis. According to the ROC analysis, SIRI had a superior diagnostic ability to neutrophil-lymphocyte ratio, platelet-lymphocyte ratio, and monocyte-lymphocyte ratio for CMD (area under the curve [AUC] =0.581) and CMM (AUC = 0.633).</p><p><strong>Conclusions: </strong>Elevated level of SIRI was positively associated with the prevalence of DM, coronary artery disease, stroke, CMD, and CMM, suggesting that SIRI could be a potential noninvasive biomarker for CMD and CMM.</p>","PeriodicalId":9288,"journal":{"name":"Brain Circulation","volume":"11 1","pages":"39-47"},"PeriodicalIF":4.8000,"publicationDate":"2025-03-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11984816/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brain Circulation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4103/bc.bc_32_24","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Chronic inflammation plays an essential role in the occurrence and progression of cardiometabolic diseases (CMDs). We aim to examine the association between a novel inflammatory biomarker Systemic Inflammatory Response Index (SIRI) and different cardiometabolic multimorbidity (CMM) statuses.
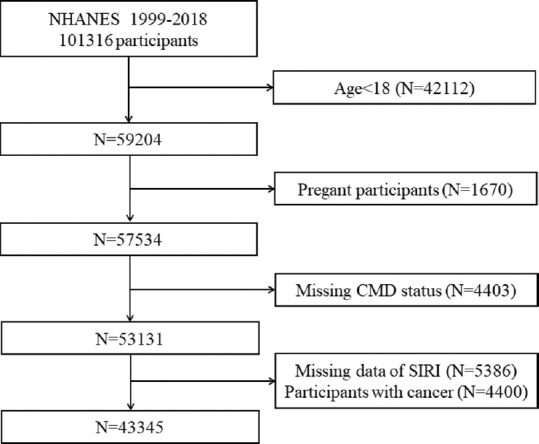
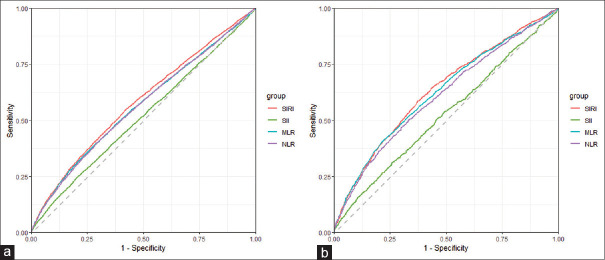
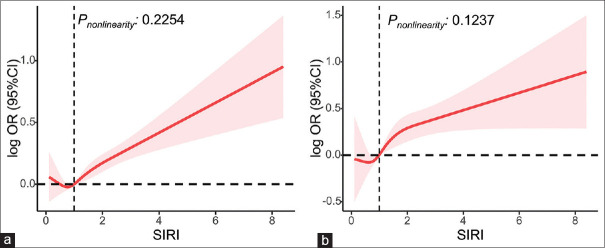
Methods: This was a cross-sectional study that includes general participants of the National Health and Nutrition Examination Survey database from 1999 to 2018. SIRI was calculated as neutrophil count × lymphocyte count/monocyte count. The CMDs were defined as a series of diseases including diabetes mellitus (DM), heart disease (HD), and stroke. We explored the association of SIRI with outcomes with weighted multivariable logistic regression models weighted restricted cubic spline. The diagnostic value of SIRI was evaluated using weighted receiver operating characteristic (ROC) curves.
Results: A total of 43,345 participants were enrolled with a mean age of 45.86 years. The weighted prevalence of CMD and CMM was 17.14% and 2.94%, respectively. Compared to those without CMD, the adjusted odds ratios (95% confidence interval) for each unit increase in SIRI were 1.14 (1.09-1.19) for DM, 1.13 (1.07-1.19) for HD, 1.11 (1.04-1.19) for stroke, 1.17 (1.12-1.22) for CMD, and 1.16 (1.10-1.23) for CMM, according to the weighted multivariable logistic regression. Elevated SIRI level was independently associated with increased CMM. There was no interaction found in subgroup analysis. According to the ROC analysis, SIRI had a superior diagnostic ability to neutrophil-lymphocyte ratio, platelet-lymphocyte ratio, and monocyte-lymphocyte ratio for CMD (area under the curve [AUC] =0.581) and CMM (AUC = 0.633).
Conclusions: Elevated level of SIRI was positively associated with the prevalence of DM, coronary artery disease, stroke, CMD, and CMM, suggesting that SIRI could be a potential noninvasive biomarker for CMD and CMM.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


