{"title":"Long-term impact of anthracycline in early-stage breast cancer, bridging of MiRNAs profiler for early cardiotoxicity.","authors":"Nattaya Poovorawan, Thiti Susiriwatananont, Chinachote Teerapakpinyo, Pajaree Chariyavilaskul, Piyada Sitthideatphaiboon, Luxica Jarutasnangkul, Monravee Tumkosit, Pairoj Chattranukulchai, Nonthikorn Theerasuwipakorn, Chatchawit Aporntewan, Shanop Shuangshoti, Sopark Manasnayakorn, Chanida Vinayanuwattikun, Yongkasem Vorasettakarnkij, Virote Sriuranpong","doi":"10.1186/s40959-025-00337-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Anthracyclines are essential in early breast cancer chemotherapy but pose long-term cardiotoxicity risks.</p><p><strong>Objectives: </strong>This study aims to investigate the long-term incidence of cancer therapy-related cardiac dysfunction (CTRCD), bridging with the miRNAs profiler representing acute cardiac injury.</p><p><strong>Methods: </strong>We conducted a prospective cohort including stage I-III breast cancer patients who received anthracycline between 2007 and 2012. Echocardiography was performed before and 12 weeks after anthracycline administration. The miRNAs profiler was conducted by NanoString and RT-PCR. Long-term cardiac magnetic resonance imaging (CMR) was evaluated in 24.2% of asymptomatic participants.</p><p><strong>Results: </strong>At a median follow-up of 11 [IQR 6-12] years, 194 patients who completed follow-up echocardiography after anthracycline were included in the analysis. The median age at diagnosis was 50 [26-72] years. An early LVEF decline of ≥ 10% was found in 32.9% of participants. The cumulative equivalent dose of doxorubicin was 223.2 ± 21.6 mg/m2. At the time of censoring, sixty-four participants (32.9%) died, 70% from breast cancer. Nine participants (4.6%) reported cardiovascular events compatible with the CTRCD definition. Forty-seven participants (24.2%) underwent long-term cardiac evaluation. The miRNAs profiler and RT-PCR at different time points, 3 weeks and 6 weeks, respectively, revealed significantly diverse expressions of miR-1-3p and miR-16-5p in participants with and without an early LVEF decline of ≥ 10%. Despite cardiac injury demonstrated by dynamic miR-1-3p and miR-16-5p, CMR parameters revealed no significant differences.</p><p><strong>Conclusions: </strong>Our study demonstrates a very low incidence of long-term symptomatic CTRCD. The diverse expression patterns of miR-16-5p and miR-1-3p at different time points also provide valuable biological insights. Within-normal results of an exact and comprehensive CMR, in asymptomatic and any LVEF change participants, indicate the long-term safety of limited-dose anthracycline-containing use.</p>","PeriodicalId":9804,"journal":{"name":"Cardio-oncology","volume":"11 1","pages":"39"},"PeriodicalIF":3.2000,"publicationDate":"2025-04-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12016148/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardio-oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40959-025-00337-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Anthracyclines are essential in early breast cancer chemotherapy but pose long-term cardiotoxicity risks.
Objectives: This study aims to investigate the long-term incidence of cancer therapy-related cardiac dysfunction (CTRCD), bridging with the miRNAs profiler representing acute cardiac injury.
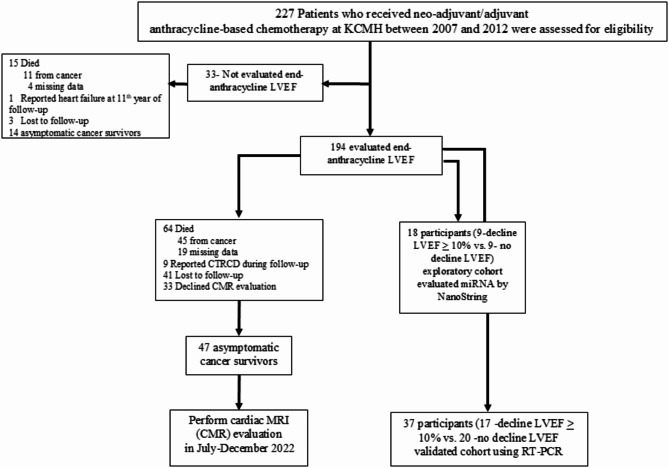
Methods: We conducted a prospective cohort including stage I-III breast cancer patients who received anthracycline between 2007 and 2012. Echocardiography was performed before and 12 weeks after anthracycline administration. The miRNAs profiler was conducted by NanoString and RT-PCR. Long-term cardiac magnetic resonance imaging (CMR) was evaluated in 24.2% of asymptomatic participants.
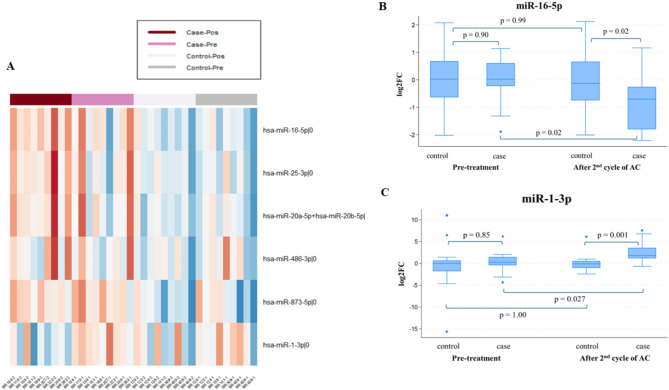
Results: At a median follow-up of 11 [IQR 6-12] years, 194 patients who completed follow-up echocardiography after anthracycline were included in the analysis. The median age at diagnosis was 50 [26-72] years. An early LVEF decline of ≥ 10% was found in 32.9% of participants. The cumulative equivalent dose of doxorubicin was 223.2 ± 21.6 mg/m2. At the time of censoring, sixty-four participants (32.9%) died, 70% from breast cancer. Nine participants (4.6%) reported cardiovascular events compatible with the CTRCD definition. Forty-seven participants (24.2%) underwent long-term cardiac evaluation. The miRNAs profiler and RT-PCR at different time points, 3 weeks and 6 weeks, respectively, revealed significantly diverse expressions of miR-1-3p and miR-16-5p in participants with and without an early LVEF decline of ≥ 10%. Despite cardiac injury demonstrated by dynamic miR-1-3p and miR-16-5p, CMR parameters revealed no significant differences.
Conclusions: Our study demonstrates a very low incidence of long-term symptomatic CTRCD. The diverse expression patterns of miR-16-5p and miR-1-3p at different time points also provide valuable biological insights. Within-normal results of an exact and comprehensive CMR, in asymptomatic and any LVEF change participants, indicate the long-term safety of limited-dose anthracycline-containing use.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


