Mathew Kunthara, Greg A Knoll, David Massicotte-Azarniouch
{"title":"Infection Risks With Thymoglobulin Use for Delayed Graft Function in Deceased Donor Kidney Transplantation: Research Letter.","authors":"Mathew Kunthara, Greg A Knoll, David Massicotte-Azarniouch","doi":"10.1177/20543581251338402","DOIUrl":null,"url":null,"abstract":"<p><p>Anti-thymocyte globulin (ATG) is often used when delayed graft function (DGF) occurs post-transplantation. The ATG may be associated with an increased risk of infections but may also decrease rejection risk in high-immunological risk recipients. The safety of ATG for the indication of DGF in low-immunological risk recipients has not been well characterized. We conducted a retrospective cohort study of deceased donor kidney transplant recipients deemed low-immunological risk and not planned for ATG induction, from June 2019 to June 2023 (N = 139). Participants switched to ATG post-transplant due to DGF (exposure; N = 68) were compared to those who did not receive ATG for induction (controls; N = 71 basiliximab only induction). Outcomes examined included BK, cytomegalovirus (CMV), and serious infection as well as acute rejection, graft loss, and death. Participants who received ATG for DGF, compared to controls, were older (63.9 vs 59.7 years), more often had diabetes as cause of kidney failure (45.5% vs 33.8%) were more often recipients of death determination by circulatory criteria donor (70.5% vs 30.9%) and extended criteria donor kidneys (48.5% vs 32.3%). There was no significant difference in the probability of BK (22.1% vs 21.1%, <i>P</i> = .89), CMV (20.6% vs 9.9%, <i>P</i> = .08), serious infections (44.1% vs 43.6%, <i>P</i> = .96), acute rejection, graft loss, or death. The use of ATG for DGF following kidney transplantation did not significantly increase infection risk nor did it improve graft outcomes. Further studies are needed to clarify the risk-benefit trade-off of using ATG for DGF.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"12 ","pages":"20543581251338402"},"PeriodicalIF":1.5000,"publicationDate":"2025-05-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12062586/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581251338402","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
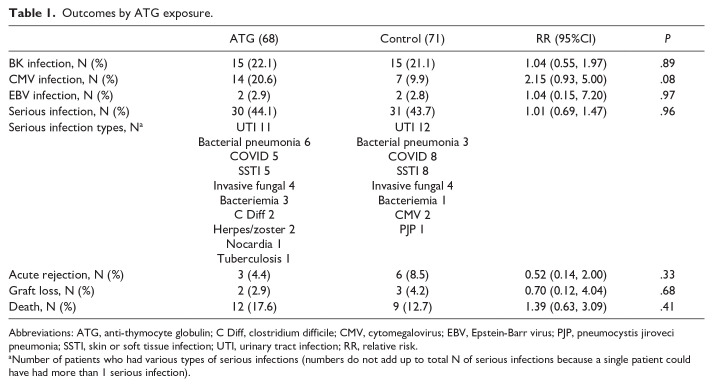
Anti-thymocyte globulin (ATG) is often used when delayed graft function (DGF) occurs post-transplantation. The ATG may be associated with an increased risk of infections but may also decrease rejection risk in high-immunological risk recipients. The safety of ATG for the indication of DGF in low-immunological risk recipients has not been well characterized. We conducted a retrospective cohort study of deceased donor kidney transplant recipients deemed low-immunological risk and not planned for ATG induction, from June 2019 to June 2023 (N = 139). Participants switched to ATG post-transplant due to DGF (exposure; N = 68) were compared to those who did not receive ATG for induction (controls; N = 71 basiliximab only induction). Outcomes examined included BK, cytomegalovirus (CMV), and serious infection as well as acute rejection, graft loss, and death. Participants who received ATG for DGF, compared to controls, were older (63.9 vs 59.7 years), more often had diabetes as cause of kidney failure (45.5% vs 33.8%) were more often recipients of death determination by circulatory criteria donor (70.5% vs 30.9%) and extended criteria donor kidneys (48.5% vs 32.3%). There was no significant difference in the probability of BK (22.1% vs 21.1%, P = .89), CMV (20.6% vs 9.9%, P = .08), serious infections (44.1% vs 43.6%, P = .96), acute rejection, graft loss, or death. The use of ATG for DGF following kidney transplantation did not significantly increase infection risk nor did it improve graft outcomes. Further studies are needed to clarify the risk-benefit trade-off of using ATG for DGF.
抗胸腺细胞球蛋白(ATG)常用于移植后发生延迟移植物功能(DGF)。ATG可能与感染风险增加有关,但也可能降低高免疫风险受体的排斥风险。ATG用于低免疫风险受体DGF适应症的安全性尚未得到很好的表征。从2019年6月至2023年6月,我们对被认为免疫风险低且未计划进行ATG诱导的已故供体肾移植受者进行了回顾性队列研究(N = 139)。由于DGF暴露,参与者在移植后改用ATG;N = 68)与未接受ATG诱导的患者(对照组;N = 71仅巴昔昔单抗诱导)。检查的结果包括BK、巨细胞病毒(CMV)、严重感染以及急性排斥反应、移植物丢失和死亡。与对照组相比,接受ATG治疗DGF的参与者年龄更大(63.9 vs 59.7岁),更常因糖尿病导致肾衰竭(45.5% vs 33.8%),更常接受循环标准供者(70.5% vs 30.9%)和扩展标准供者肾脏(48.5% vs 32.3%)的死亡测定。BK (22.1% vs 21.1%, P = 0.89)、CMV (20.6% vs 9.9%, P = 0.08)、严重感染(44.1% vs 43.6%, P = 0.96)、急性排斥反应、移植物丢失或死亡的概率无显著差异。肾移植后使用ATG进行DGF治疗并没有显著增加感染风险,也没有改善移植结果。需要进一步的研究来阐明使用ATG治疗DGF的风险-收益权衡。
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


