Planning evaluation of stereotactic magnetic resonance-guided online adaptive radiosurgery for kidney tumors close to the organ at risk: is it valuable to wait for good timing to perform stereotactic radiosurgery?
{"title":"Planning evaluation of stereotactic magnetic resonance-guided online adaptive radiosurgery for kidney tumors close to the organ at risk: is it valuable to wait for good timing to perform stereotactic radiosurgery?","authors":"Takaya Yamamoto, Shohei Tanaka, Noriyoshi Takahashi, Rei Umezawa, Yu Suzuki, Keita Kishida, So Omata, Kazuya Takeda, Hinako Harada, Kiyokazu Sato, Yoshiyuki Katsuta, Noriyuki Kadoya, Keiichi Jingu","doi":"10.3857/roj.2024.00521","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This study aimed to investigate changes in target coverage using magnetic resonance-guided online adaptive radiotherapy (MRgoART) for kidney tumors and to evaluate the suitable timing of treatment.</p><p><strong>Materials and methods: </strong>Among patients treated with 3-fraction MRgoART for kidney cancer, 18 tumors located within 1 cm of the gastrointestinal tract were selected. Stereotactic radiosurgery planning with a prescription dose of 26 Gy was performed using pretreatment simulation and three MRgoART timings with an adapt-to-shape method. The best MRgoART plan was defined as the plan achieving the highest percentage of planning target volume (PTV) coverage of 26 Gy. In clinical scenario simulation, MRgoART plans were evaluated in the order of actual treatment. Waiting for the next timing was done when the PTV coverage of 26 Gy did not achieve 95%-99% or did not increase by 5% or more compared to the pretreatment plan.</p><p><strong>Results: </strong>The median percentages of PTV receiving 26 Gy in pretreatment and the first, second, and third MRgoART were 82% (range, 19%), 63% (range, 7% to 99%), 88% (range, 31% to 99%), and 95% (range, 3% to 99%), respectively. Comparing pretreatment simulation plans with the best MRgoART plans showed a significant difference (p = 0.025). In the clinical scenario simulation, 16 of the 18 planning series, including nine plans with 95%-99% PTV coverage of 26 Gy and seven plans with increased PTV coverage by 5% or more, would be irradiated at a good timing.</p><p><strong>Conclusion: </strong>MRgoART revealed dose coverage differences at each MRgoART timing. Waiting for optimal irradiation timing could be an option in case of suboptimal timing.</p>","PeriodicalId":94184,"journal":{"name":"Radiation oncology journal","volume":"43 1","pages":"40-48"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12010889/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiation oncology journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3857/roj.2024.00521","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/17 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: This study aimed to investigate changes in target coverage using magnetic resonance-guided online adaptive radiotherapy (MRgoART) for kidney tumors and to evaluate the suitable timing of treatment.
Materials and methods: Among patients treated with 3-fraction MRgoART for kidney cancer, 18 tumors located within 1 cm of the gastrointestinal tract were selected. Stereotactic radiosurgery planning with a prescription dose of 26 Gy was performed using pretreatment simulation and three MRgoART timings with an adapt-to-shape method. The best MRgoART plan was defined as the plan achieving the highest percentage of planning target volume (PTV) coverage of 26 Gy. In clinical scenario simulation, MRgoART plans were evaluated in the order of actual treatment. Waiting for the next timing was done when the PTV coverage of 26 Gy did not achieve 95%-99% or did not increase by 5% or more compared to the pretreatment plan.
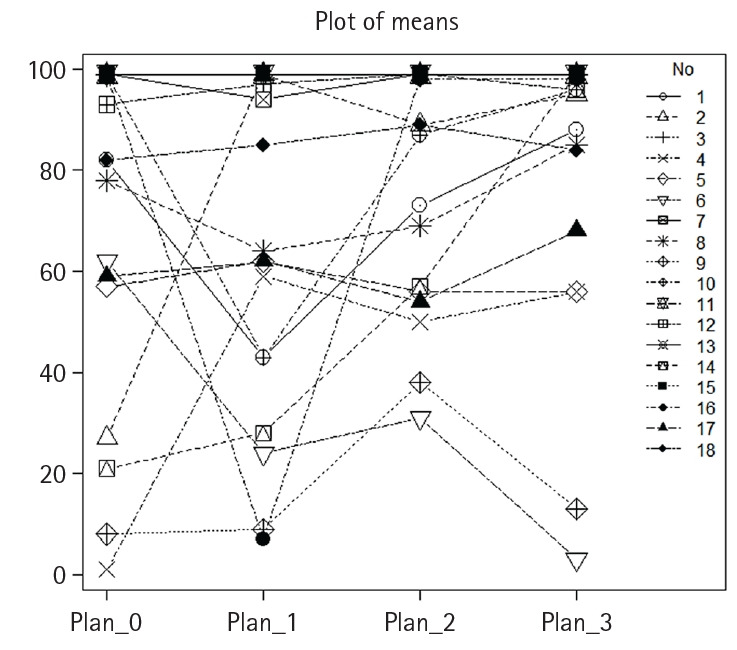
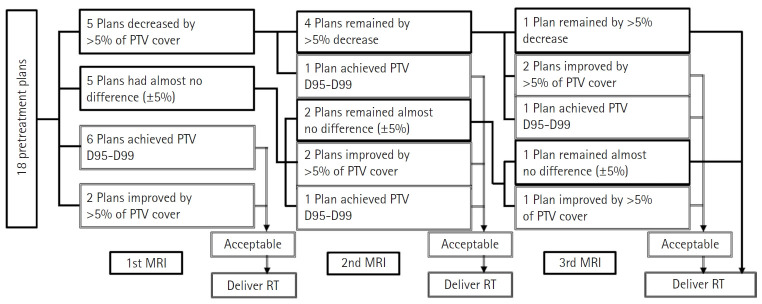
Results: The median percentages of PTV receiving 26 Gy in pretreatment and the first, second, and third MRgoART were 82% (range, 19%), 63% (range, 7% to 99%), 88% (range, 31% to 99%), and 95% (range, 3% to 99%), respectively. Comparing pretreatment simulation plans with the best MRgoART plans showed a significant difference (p = 0.025). In the clinical scenario simulation, 16 of the 18 planning series, including nine plans with 95%-99% PTV coverage of 26 Gy and seven plans with increased PTV coverage by 5% or more, would be irradiated at a good timing.
Conclusion: MRgoART revealed dose coverage differences at each MRgoART timing. Waiting for optimal irradiation timing could be an option in case of suboptimal timing.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


