José Fernando Gómez-Urrego, Nathalie Yepes-Madrid, Mónica Alexandra Gil-Artunduaga, María Del Pilar Gómez-Mora, Luis Fernando Mejía-Rivera, Robinson Pacheco-López, Juan Pablo Rojas-Hernández
{"title":"Bacterial infection in patients with juvenile systemic lupus erythematosus and fever.","authors":"José Fernando Gómez-Urrego, Nathalie Yepes-Madrid, Mónica Alexandra Gil-Artunduaga, María Del Pilar Gómez-Mora, Luis Fernando Mejía-Rivera, Robinson Pacheco-López, Juan Pablo Rojas-Hernández","doi":"10.1186/s12969-025-01088-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Juvenile Systemic Lupus Erythematosus (JSLE) is a chronic, systemic autoimmune disease characterized by an increased susceptibility to infections. Fever in these patients can result from infection, heightened lupus activity, or a combination of both. Various clinical factors and biomarkers have been proposed to differentiate between infection and disease activity, but the results remain inconclusive. The Systemic Lupus Erythematosus Disease Activity Index-2000 (SLEDAI-2 k) is used to assess lupus activity in the presence or absence of infection. This study aimed to identify factors associated with bacterial infections in JSLE patients presenting with fever.</p><p><strong>Methods: </strong>A case-control study, approved by the institutional ethics committee, was conducted.</p><p><strong>Results: </strong>Bacterial infection was identified in 17% of 116 patients. Factors evaluated included immunomodulator use, high-dose steroids, renal replacement therapy, erythrocyte sedimentation rate (ESR) > 20, C-reactive protein (CRP) > 60 and > 90 mg/L, ferritin > 500 ng/mL, neutrophil-to-lymphocyte ratio (NLR) > 6, platelet-to-lymphocyte ratio (PLR) > 133, procalcitonin (PCT) > 0.9 ng/mL, lymphocyte-to-C4 ratio (LC4R) > 66.7, and ESR/CRP ratio < 2. In the adjusted model, PCT > 0.9 ng/mL retained significance with p < 0.01. Nagelkerke's R<sup>2</sup> was 0.65, and the Hosmer-Lemeshow test indicated good internal validity.</p><p><strong>Conclusions: </strong>Bacterial infection was detected in 17% of JSLE patients with fever. Procalcitonin > 0.9 ng/mL is a critical marker for identifying bacterial infection. NLR, PLR, ESR/CRP ratio, LC4R, and ferritin require further investigation to establish definitive cut-off values for differentiating bacterial infections from other infections or disease activity. Individual patient evaluation remains the recommended approach for diagnosis.</p>","PeriodicalId":54630,"journal":{"name":"Pediatric Rheumatology","volume":"23 1","pages":"39"},"PeriodicalIF":2.3000,"publicationDate":"2025-04-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11980166/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Rheumatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12969-025-01088-1","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Juvenile Systemic Lupus Erythematosus (JSLE) is a chronic, systemic autoimmune disease characterized by an increased susceptibility to infections. Fever in these patients can result from infection, heightened lupus activity, or a combination of both. Various clinical factors and biomarkers have been proposed to differentiate between infection and disease activity, but the results remain inconclusive. The Systemic Lupus Erythematosus Disease Activity Index-2000 (SLEDAI-2 k) is used to assess lupus activity in the presence or absence of infection. This study aimed to identify factors associated with bacterial infections in JSLE patients presenting with fever.
Methods: A case-control study, approved by the institutional ethics committee, was conducted.
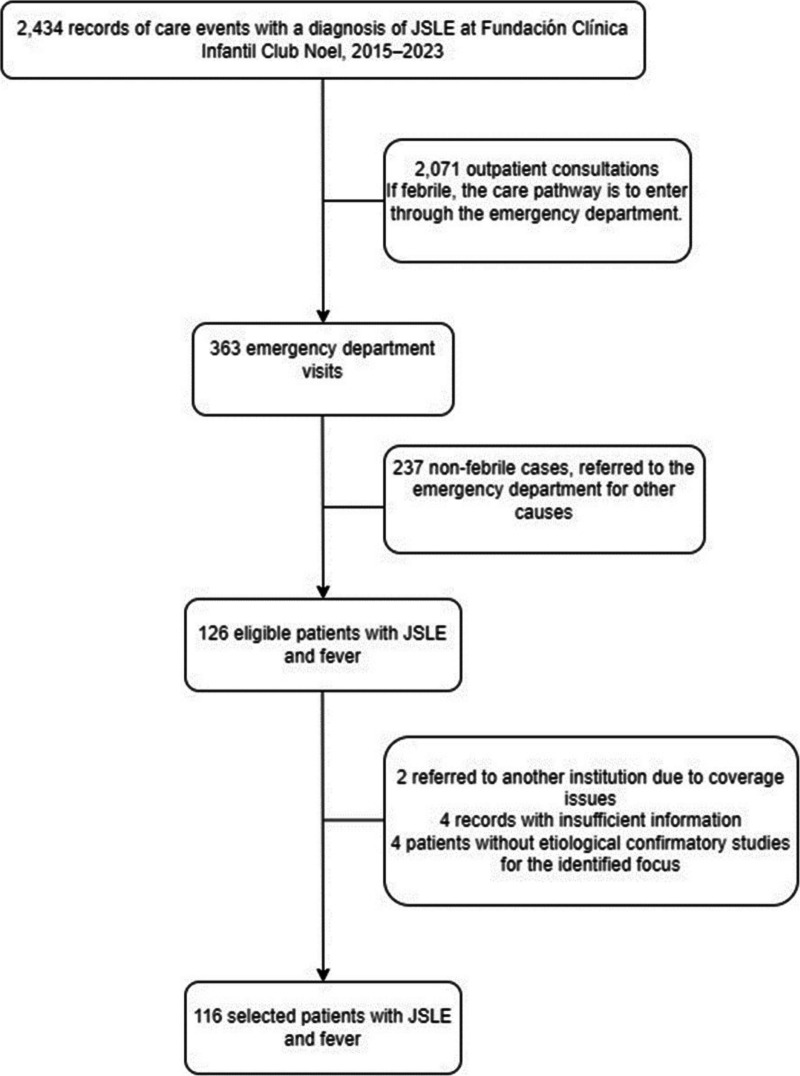
Results: Bacterial infection was identified in 17% of 116 patients. Factors evaluated included immunomodulator use, high-dose steroids, renal replacement therapy, erythrocyte sedimentation rate (ESR) > 20, C-reactive protein (CRP) > 60 and > 90 mg/L, ferritin > 500 ng/mL, neutrophil-to-lymphocyte ratio (NLR) > 6, platelet-to-lymphocyte ratio (PLR) > 133, procalcitonin (PCT) > 0.9 ng/mL, lymphocyte-to-C4 ratio (LC4R) > 66.7, and ESR/CRP ratio < 2. In the adjusted model, PCT > 0.9 ng/mL retained significance with p < 0.01. Nagelkerke's R2 was 0.65, and the Hosmer-Lemeshow test indicated good internal validity.
Conclusions: Bacterial infection was detected in 17% of JSLE patients with fever. Procalcitonin > 0.9 ng/mL is a critical marker for identifying bacterial infection. NLR, PLR, ESR/CRP ratio, LC4R, and ferritin require further investigation to establish definitive cut-off values for differentiating bacterial infections from other infections or disease activity. Individual patient evaluation remains the recommended approach for diagnosis.
期刊介绍:
Pediatric Rheumatology is an open access, peer-reviewed, online journal encompassing all aspects of clinical and basic research related to pediatric rheumatology and allied subjects.
The journal’s scope of diseases and syndromes include musculoskeletal pain syndromes, rheumatic fever and post-streptococcal syndromes, juvenile idiopathic arthritis, systemic lupus erythematosus, juvenile dermatomyositis, local and systemic scleroderma, Kawasaki disease, Henoch-Schonlein purpura and other vasculitides, sarcoidosis, inherited musculoskeletal syndromes, autoinflammatory syndromes, and others.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


