Nadia Corcione, Alfonso Pecoraro, Andrea Fidecicchi, Severo Campione, Lina Zuccatosta, Giuseppe Failla
{"title":"Transbronchial Mediastinal Cryobiopsy Diagnostic Yield and Perioperative Patient Management: A Single Tertiary Center Experience.","authors":"Nadia Corcione, Alfonso Pecoraro, Andrea Fidecicchi, Severo Campione, Lina Zuccatosta, Giuseppe Failla","doi":"10.4274/ThoracResPract.2025.2024-12-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) is widely used to diagnose mediastinal lesions; however, small cytology samples from EBUS-TBNA may be inadequate in cases of benign lung diseases, hematologic disorders, and to assess the molecular profile of primary lung cancer (PLC). EBUS-guided transbronchial mediastinal cryobiopsy (TMC) obtains histological samples and potentially implies a higher diagnostic yield (DY) than EBUS-TBNA. The clinical impact of this technique and the perioperative patient management are still unclear. Our aim was to critically analyze our experience with TMC.</p><p><strong>Material and methods: </strong>A single center retrospective study was conducted to evaluate TMC DY and perioperative routine over 11 months (February 2023-January 2024).</p><p><strong>Results: </strong>Forty-one patients were included. The overall DY was 41.5% and 95.1% for EBUS-TBNA and TMC, respectively. TMC provided a higher DY than EBUS-TBNA in cases of hematologic disorders, benign diseases, and uncommon tumors (31% for EBUS-TBNA and 100% for TMC; 95% confidence interval (CI): 52.1-85.8, <i>P</i> < 0.001). For PLC, the DY and the assessment of immunohistochemical marker expression did not significantly differ between the two techniques (80% for EBUS-TBNA and 100% for TMC; 95% CI: -4.79-44.8, <i>P</i> = 0.13). The management of antithrombotic therapy was the same as that of EBUS-TBNA. Sedatives were administered to achieve deep sedation. After the procedure, no step-up in the level of care was observed, either in outpatients or in patients with a Charlson Comorbidity Index ≥5.</p><p><strong>Conclusion: </strong>TMC had a better DY than EBUS-TBNA in hematologic disorders, benign lung disease, and uncommon tumors, with an optimal tolerability profile.</p>","PeriodicalId":75221,"journal":{"name":"Thoracic research and practice","volume":" ","pages":"183-190"},"PeriodicalIF":0.6000,"publicationDate":"2025-06-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12243428/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Thoracic research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4274/ThoracResPract.2025.2024-12-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/8 0:00:00","PubModel":"Epub","JCR":"0","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) is widely used to diagnose mediastinal lesions; however, small cytology samples from EBUS-TBNA may be inadequate in cases of benign lung diseases, hematologic disorders, and to assess the molecular profile of primary lung cancer (PLC). EBUS-guided transbronchial mediastinal cryobiopsy (TMC) obtains histological samples and potentially implies a higher diagnostic yield (DY) than EBUS-TBNA. The clinical impact of this technique and the perioperative patient management are still unclear. Our aim was to critically analyze our experience with TMC.
Material and methods: A single center retrospective study was conducted to evaluate TMC DY and perioperative routine over 11 months (February 2023-January 2024).
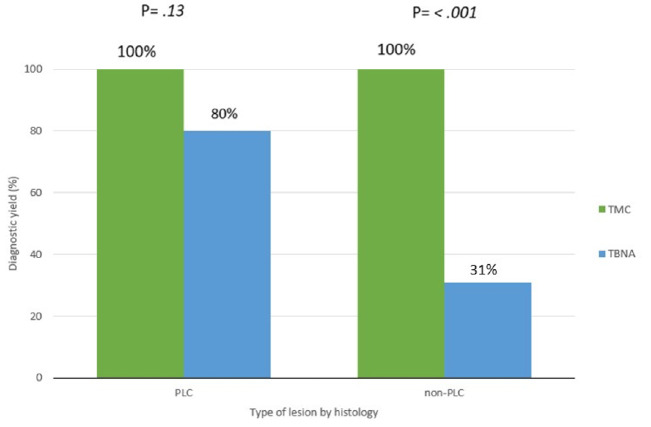
Results: Forty-one patients were included. The overall DY was 41.5% and 95.1% for EBUS-TBNA and TMC, respectively. TMC provided a higher DY than EBUS-TBNA in cases of hematologic disorders, benign diseases, and uncommon tumors (31% for EBUS-TBNA and 100% for TMC; 95% confidence interval (CI): 52.1-85.8, P < 0.001). For PLC, the DY and the assessment of immunohistochemical marker expression did not significantly differ between the two techniques (80% for EBUS-TBNA and 100% for TMC; 95% CI: -4.79-44.8, P = 0.13). The management of antithrombotic therapy was the same as that of EBUS-TBNA. Sedatives were administered to achieve deep sedation. After the procedure, no step-up in the level of care was observed, either in outpatients or in patients with a Charlson Comorbidity Index ≥5.
Conclusion: TMC had a better DY than EBUS-TBNA in hematologic disorders, benign lung disease, and uncommon tumors, with an optimal tolerability profile.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


