Single-session intervention with and without video support to prevent the worsening of emotional distress among healthcare workers during the SARS-CoV-2 pandemic: a randomised clinical trial.
Giovanni Abrahão Salum, Lucas Spanemberg, Marianna de Abreu Costa, André Rafael Simioni, Natan Pereira Gosmann, Livia Hartmann de Souza, Pim Cuijpers, Daniel Samuel Pine, Andre Russowsky Brunoni, Natan Katz, Roberto Nunes Umpierre, Christian Haag Kristensen, Gisele Gus Manfro, Marcelo Pio Fleck, Carolina Blaya Dreher
{"title":"Single-session intervention with and without video support to prevent the worsening of emotional distress among healthcare workers during the SARS-CoV-2 pandemic: a randomised clinical trial.","authors":"Giovanni Abrahão Salum, Lucas Spanemberg, Marianna de Abreu Costa, André Rafael Simioni, Natan Pereira Gosmann, Livia Hartmann de Souza, Pim Cuijpers, Daniel Samuel Pine, Andre Russowsky Brunoni, Natan Katz, Roberto Nunes Umpierre, Christian Haag Kristensen, Gisele Gus Manfro, Marcelo Pio Fleck, Carolina Blaya Dreher","doi":"10.1136/bmjment-2024-301416","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The SARS-CoV-2 pandemic was a major stressful event that significantly affected healthcare providers.</p><p><strong>Objective: </strong>To evaluate the efficacy of a single-session intervention (SSI), with and without weekly personalised prerecorded videos, in preventing emotional distress worsening.</p><p><strong>Methods: </strong>Nationwide randomised clinical trial conducted in Brazil from 19 May 2020 to 31 December 2021. We included healthcare professionals with anxiety, depression or irritability scores below a T-score of 70, measured by the Patient-Reported Outcomes Measurement Information System. Participants were randomised to SSI or SSI plus weekly personalised prerecorded videos for 4 weeks (SSI-ET). The primary outcome was the proportion of participants with a significant escalation of symptoms (ie, T-score above 70).</p><p><strong>Findings: </strong>From 3328 assessed for eligibility, 1112 participants were randomised (SSI=549; SSI-ET=563). The cumulative proportion of incident cases at 6 months was 17.5% (95% CI: 13.1% to 21.6%) for SSI and 15% (95% CI: 10.9% to 18.8%) for SSI-ET, with no difference between groups (HR=0.81, 95% CI: 0.83 to 1.79). Both groups showed significant symptom reductions at 1 month follow-up, maintained at 3 and 6 months (Cohen's d=0.68-1.08).</p><p><strong>Conclusions: </strong>Adding asynchronous videos to SSI provided no additional benefit. While symptom improvements occurred over time, the lack of a control group limits conclusions about intervention efficacy.</p><p><strong>Clinical implications: </strong>Given its simplicity and scalability, the synchronous component, which includes core mental health support elements, such as active listening, validation, and empathic care, may represent a feasible way to assist healthcare professionals in crisis settings, even though further research is needed to determine its specific impact.</p><p><strong>Trial registration number: </strong>NCT04632082.</p>","PeriodicalId":72434,"journal":{"name":"BMJ mental health","volume":"28 1","pages":""},"PeriodicalIF":4.9000,"publicationDate":"2025-04-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11977485/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ mental health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjment-2024-301416","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"0","JCRName":"PSYCHIATRY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The SARS-CoV-2 pandemic was a major stressful event that significantly affected healthcare providers.
Objective: To evaluate the efficacy of a single-session intervention (SSI), with and without weekly personalised prerecorded videos, in preventing emotional distress worsening.
Methods: Nationwide randomised clinical trial conducted in Brazil from 19 May 2020 to 31 December 2021. We included healthcare professionals with anxiety, depression or irritability scores below a T-score of 70, measured by the Patient-Reported Outcomes Measurement Information System. Participants were randomised to SSI or SSI plus weekly personalised prerecorded videos for 4 weeks (SSI-ET). The primary outcome was the proportion of participants with a significant escalation of symptoms (ie, T-score above 70).
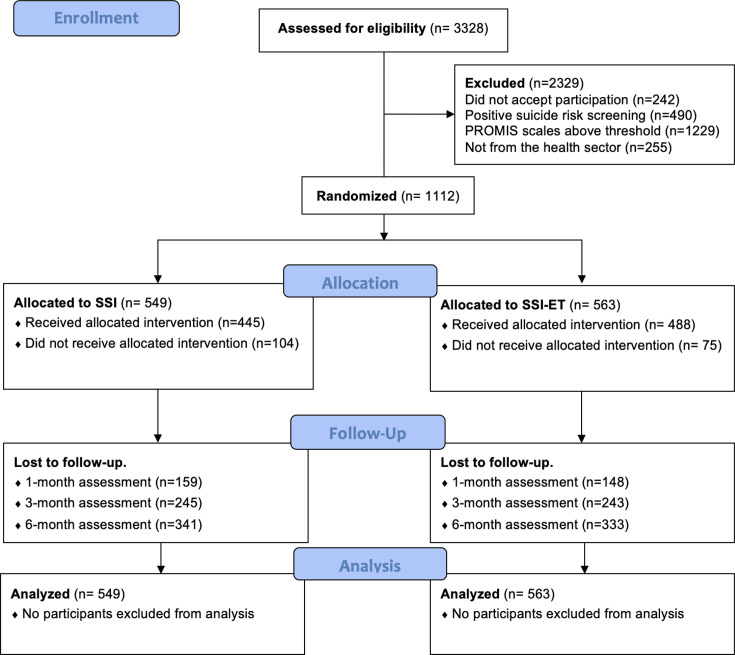
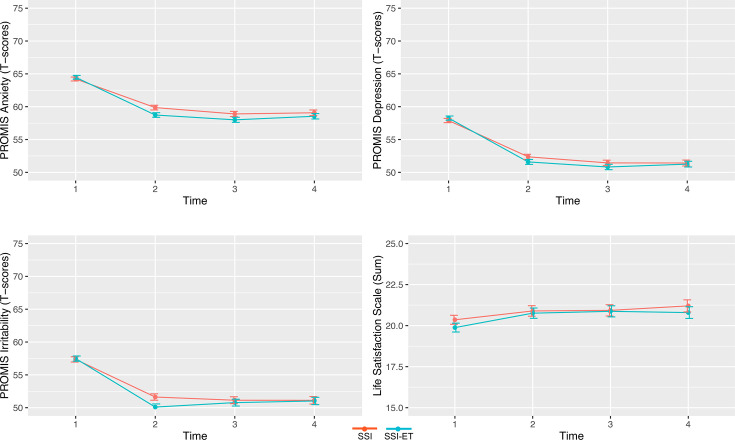
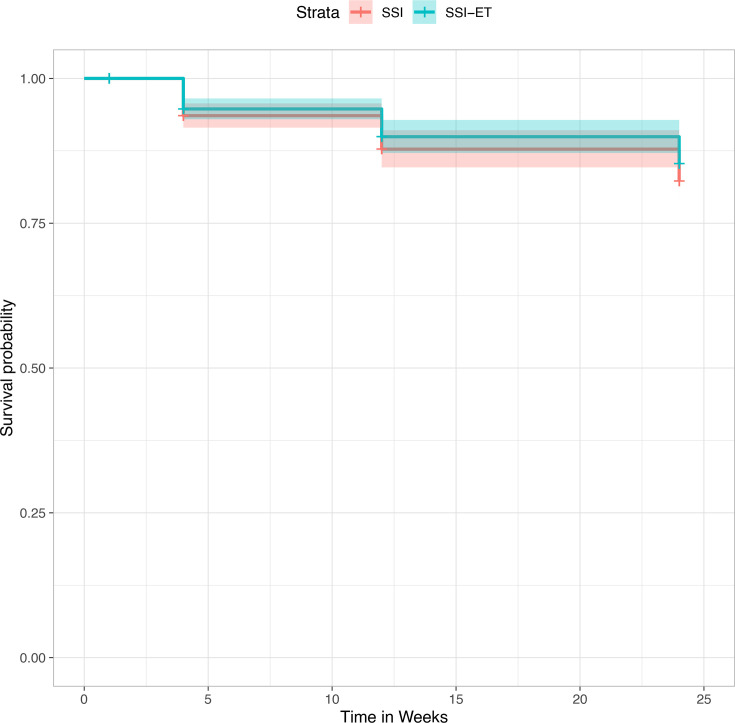
Findings: From 3328 assessed for eligibility, 1112 participants were randomised (SSI=549; SSI-ET=563). The cumulative proportion of incident cases at 6 months was 17.5% (95% CI: 13.1% to 21.6%) for SSI and 15% (95% CI: 10.9% to 18.8%) for SSI-ET, with no difference between groups (HR=0.81, 95% CI: 0.83 to 1.79). Both groups showed significant symptom reductions at 1 month follow-up, maintained at 3 and 6 months (Cohen's d=0.68-1.08).
Conclusions: Adding asynchronous videos to SSI provided no additional benefit. While symptom improvements occurred over time, the lack of a control group limits conclusions about intervention efficacy.
Clinical implications: Given its simplicity and scalability, the synchronous component, which includes core mental health support elements, such as active listening, validation, and empathic care, may represent a feasible way to assist healthcare professionals in crisis settings, even though further research is needed to determine its specific impact.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


