Min-Jie Low, Zhen Yi Liau, Jun Leong Cheong, Pui San Loh, Ina Ismiarti Shariffuddin, Hui Min Khor
{"title":"Impact of Physical and Cognitive Frailty on Long-Term Mortality in Older Patients undergoing Elective Non-cardiac Surgery.","authors":"Min-Jie Low, Zhen Yi Liau, Jun Leong Cheong, Pui San Loh, Ina Ismiarti Shariffuddin, Hui Min Khor","doi":"10.4235/agmr.24.0163","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Older adults undergoing surgery frequently have multiple comorbidities and reduced physical and cognitive reserves. This study aims to assess the effect of physical and cognitive frailty on long-term mortality in older patients undergoing elective non-cardiac surgery in a tertiary center.</p><p><strong>Methods: </strong>Patients aged ≥65 years old admitted to surgical wards at the University of Malaya Medical Centre were recruited. Physical frailty and cognitive status were assessed using the Fried Frailty Index (FFI) and the Montreal Cognitive Assessment, respectively. Patients were stratified into six groups based on their frailty and cognitive status: Group 1, normal cognition and non-frail (reference group); Group 2, normal cognition and frail; Group 3, mild cognitive impairment (MCI) and non-frail; Group 4, MCI and frail; Group 5, dementia and non-frail; and Group 6, dementia and frail.</p><p><strong>Results: </strong>A total of 406 patients with a mean FFI score of 1.1±1.2 were recruited. Predictors of mortality include male sex (hazard ratio [HR]=1.96; 95% confidence interval [CI], 1.14-3.37; p=0.015), presence of active malignancy (HR=3.86; 95% CI, 2.14-6.95; p<0.001), and high FFI scores (1.8±1.2 vs. 1.0±1.1; p=0.013). Compared to Group 1, long-term mortality risk was significantly increased in Group 4 (HR=3.17; 95% CI, 1.36-7.38) and Group 6 (HR=3.91; 95% CI, 1.62-9.43) patients.</p><p><strong>Conclusion: </strong>The combination of physical frailty and cognitive impairment was associated with long-term mortality risk among older patients who underwent elective non-cardiac surgery. This highlights the importance of assessing physical frailty and cognitive function of all older surgical patients to guide targeted intervention, especially for those with impairments which may be potentially reversible.</p>","PeriodicalId":44729,"journal":{"name":"Annals of Geriatric Medicine and Research","volume":"29 1","pages":"111-118"},"PeriodicalIF":3.2000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12010741/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Geriatric Medicine and Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4235/agmr.24.0163","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/17 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Older adults undergoing surgery frequently have multiple comorbidities and reduced physical and cognitive reserves. This study aims to assess the effect of physical and cognitive frailty on long-term mortality in older patients undergoing elective non-cardiac surgery in a tertiary center.
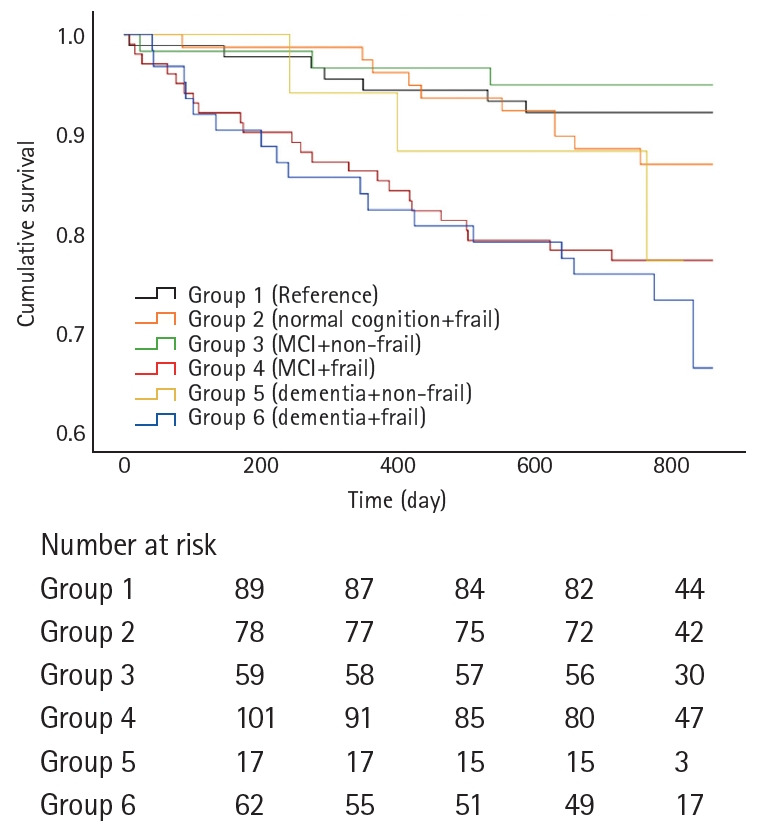
Methods: Patients aged ≥65 years old admitted to surgical wards at the University of Malaya Medical Centre were recruited. Physical frailty and cognitive status were assessed using the Fried Frailty Index (FFI) and the Montreal Cognitive Assessment, respectively. Patients were stratified into six groups based on their frailty and cognitive status: Group 1, normal cognition and non-frail (reference group); Group 2, normal cognition and frail; Group 3, mild cognitive impairment (MCI) and non-frail; Group 4, MCI and frail; Group 5, dementia and non-frail; and Group 6, dementia and frail.
Results: A total of 406 patients with a mean FFI score of 1.1±1.2 were recruited. Predictors of mortality include male sex (hazard ratio [HR]=1.96; 95% confidence interval [CI], 1.14-3.37; p=0.015), presence of active malignancy (HR=3.86; 95% CI, 2.14-6.95; p<0.001), and high FFI scores (1.8±1.2 vs. 1.0±1.1; p=0.013). Compared to Group 1, long-term mortality risk was significantly increased in Group 4 (HR=3.17; 95% CI, 1.36-7.38) and Group 6 (HR=3.91; 95% CI, 1.62-9.43) patients.
Conclusion: The combination of physical frailty and cognitive impairment was associated with long-term mortality risk among older patients who underwent elective non-cardiac surgery. This highlights the importance of assessing physical frailty and cognitive function of all older surgical patients to guide targeted intervention, especially for those with impairments which may be potentially reversible.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


