Johan van Koll, Madelon D E A Engels, Jesse H J Rijks, Madelon Salari, Jelle Luijten, Joost Lumens, Vanessa P M van Empel, Sjoerd W Westra, Antonius M W van Stipdonk, Theo A R Lankveld, Sevasti M Chaldoupi, Jacqueline Joza, Rypko J Beukema, Justin G L M Luermans, Dominik K Linz, Kevin Vernooy
{"title":"Long-term outcomes of pace-and-ablate strategy in patients with atrial fibrillation.","authors":"Johan van Koll, Madelon D E A Engels, Jesse H J Rijks, Madelon Salari, Jelle Luijten, Joost Lumens, Vanessa P M van Empel, Sjoerd W Westra, Antonius M W van Stipdonk, Theo A R Lankveld, Sevasti M Chaldoupi, Jacqueline Joza, Rypko J Beukema, Justin G L M Luermans, Dominik K Linz, Kevin Vernooy","doi":"10.1007/s10840-025-02038-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The pace-and-ablate strategy is second -line therapy to obtain rate control in patients with persistent symptomatic atrial fibrillation (AF) when other treatment options fail. This study aims to evaluate long-term effects on clinical outcomes following pace-and-ablate strategy in AF patients.</p><p><strong>Methods: </strong>This retrospective study includes patients who underwent successful pacemaker implantation (right ventricular pacing (RVP) or cardiac re-synchronization therapy (CRT)) followed by atrioventricular node ablation (AVNA) between 2010 and 2020. Patients were treated according to the prevailing guidelines. The primary endpoint was a composite of all-cause mortality and heart failure hospitalization (HFH). Secondary endpoints were individual outcomes of all-cause mortality, HFH, and left-ventricular ejection fraction (LVEF) change.</p><p><strong>Results: </strong>Two hundred ninety-eight patients were included, 162 undergoing RVP, and 136 receiving CRT, with a median follow-up of 5.8 years [4.1-8.0]. The primary endpoint occured in 47% of the RVP group and 49% of the CRT group (p = 0.206). All-cause mortality occurred in 36% of the RVP group and in 45% of the CRT group (p = 0.005). HFH occurred in 22% of the RVP group and in 15% of the CRT group (p = 0.328), with 17(10%) upgrades to CRT in the RVP group. Median LVEF in the RVP group remained stable (56% [49-60] to 53% [43-57]; p = 0.081), while it improved in the CRT group (31% [22-38] to 43% [32-51]; p < 0.001).</p><p><strong>Conclusion: </strong>Mortality and HFH in patients with AF managed through a pace-and-ablate strategy are high. Reassuringly, LVEF deterioration requiring upgrade to CRT is uncommon in patients undergoing RVP with normal baseline LVEF before AVNA. CRT improves LVEF in patients with reduced LVEF before AVNA.</p>","PeriodicalId":16202,"journal":{"name":"Journal of Interventional Cardiac Electrophysiology","volume":" ","pages":"1487-1495"},"PeriodicalIF":2.6000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12436554/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Interventional Cardiac Electrophysiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10840-025-02038-3","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/7 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The pace-and-ablate strategy is second -line therapy to obtain rate control in patients with persistent symptomatic atrial fibrillation (AF) when other treatment options fail. This study aims to evaluate long-term effects on clinical outcomes following pace-and-ablate strategy in AF patients.
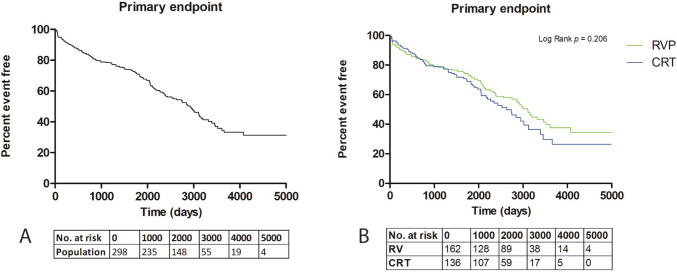
Methods: This retrospective study includes patients who underwent successful pacemaker implantation (right ventricular pacing (RVP) or cardiac re-synchronization therapy (CRT)) followed by atrioventricular node ablation (AVNA) between 2010 and 2020. Patients were treated according to the prevailing guidelines. The primary endpoint was a composite of all-cause mortality and heart failure hospitalization (HFH). Secondary endpoints were individual outcomes of all-cause mortality, HFH, and left-ventricular ejection fraction (LVEF) change.
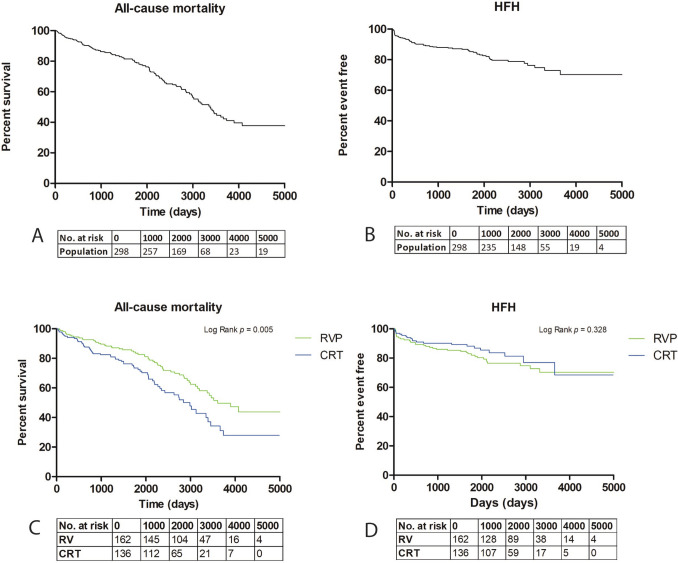
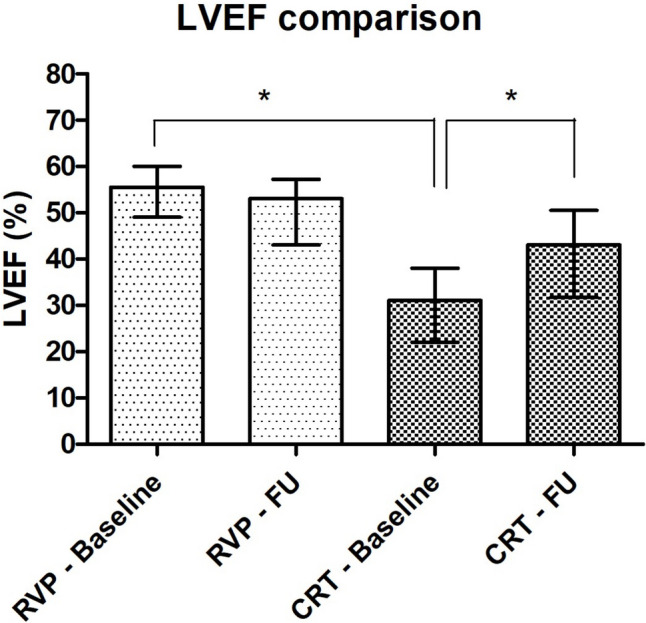
Results: Two hundred ninety-eight patients were included, 162 undergoing RVP, and 136 receiving CRT, with a median follow-up of 5.8 years [4.1-8.0]. The primary endpoint occured in 47% of the RVP group and 49% of the CRT group (p = 0.206). All-cause mortality occurred in 36% of the RVP group and in 45% of the CRT group (p = 0.005). HFH occurred in 22% of the RVP group and in 15% of the CRT group (p = 0.328), with 17(10%) upgrades to CRT in the RVP group. Median LVEF in the RVP group remained stable (56% [49-60] to 53% [43-57]; p = 0.081), while it improved in the CRT group (31% [22-38] to 43% [32-51]; p < 0.001).
Conclusion: Mortality and HFH in patients with AF managed through a pace-and-ablate strategy are high. Reassuringly, LVEF deterioration requiring upgrade to CRT is uncommon in patients undergoing RVP with normal baseline LVEF before AVNA. CRT improves LVEF in patients with reduced LVEF before AVNA.
期刊介绍:
The Journal of Interventional Cardiac Electrophysiology is an international publication devoted to fostering research in and development of interventional techniques and therapies for the management of cardiac arrhythmias. It is designed primarily to present original research studies and scholarly scientific reviews of basic and applied science and clinical research in this field. The Journal will adopt a multidisciplinary approach to link physical, experimental, and clinical sciences as applied to the development of and practice in interventional electrophysiology. The Journal will examine techniques ranging from molecular, chemical and pharmacologic therapies to device and ablation technology. Accordingly, original research in clinical, epidemiologic and basic science arenas will be considered for publication. Applied engineering or physical science studies pertaining to interventional electrophysiology will be encouraged. The Journal is committed to providing comprehensive and detailed treatment of major interventional therapies and innovative techniques in a structured and clinically relevant manner. It is directed at clinical practitioners and investigators in the rapidly growing field of interventional electrophysiology. The editorial staff and board reflect this bias and include noted international experts in this area with a wealth of expertise in basic and clinical investigation. Peer review of all submissions, conflict of interest guidelines and periodic editorial board review of all Journal policies have been established.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


