Long-term effectiveness and safety of methotrexate-tacrolimus combination therapy versus methotrexate monotherapy in reducing rheumatoid arthritis flares after TNF inhibitor discontinuation: a retrospective cohort study.
{"title":"Long-term effectiveness and safety of methotrexate-tacrolimus combination therapy versus methotrexate monotherapy in reducing rheumatoid arthritis flares after TNF inhibitor discontinuation: a retrospective cohort study.","authors":"Taio Naniwa, Mikiko Kajiura","doi":"10.1186/s41927-025-00489-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study evaluates the long-term effectiveness and safety of methotrexate-tacrolimus combination therapy compared to methotrexate monotherapy in maintaining successful tumor necrosis factor (TNF) inhibitor discontinuation in rheumatoid arthritis (RA) patients.</p><p><strong>Methods: </strong>We retrospectively analyzed consecutive RA patients who discontinued TNF inhibitors after achieving disease control by October 2022 and received either methotrexate monotherapy or methotrexate-tacrolimus combination therapy for up to 10 years. Per-observation time-to-event analyses assessed treatment failure, treatment intensification, first disease flare, and irreversible functional deterioration. Mixed-effects Cox models, time-dependent Cox models without random effects, and Kaplan-Meier estimates with inverse probability weighting were applied. Safety assessment included treatment-limiting adverse events and renal function trends.</p><p><strong>Results: </strong>A total of 147 treatment lines (96 methotrexate monotherapy and 51 combination therapy) in 116 patients were analyzed. The combination therapy significantly reduced treatment failure (hazard ratio [HR], 0.42; 95% confidence interval [CI], 0.24-0.72), treatment intensification with the index drugs (HR, 0.38; 95% CI, 0.22-0.67) and with biologics or Janus kinase inhibitors (HR, 0.39; 95% CI, 0.22-0.71), and first flare (HR, 0.55; 95%CI 0.36-0.84), with consistent findings across models. The benefit was most pronounced in patients with prior flares during methotrexate monotherapy after TNF inhibitor discontinuation, with HRs as low as 0.04-0.12 across outcomes. No significant differences in treatment-limiting adverse events were observed. The annual increase in serum creatinine for tacrolimus users was 0.0032 mg/dL, suggesting minimal long-term renal impact.</p><p><strong>Conclusions: </strong>Methotrexate-tacrolimus combination therapy significantly reduces relapse risk following TNF inhibitor discontinuation without compromising safety, offering a potentially sustainable treatment alternative after achieving remission with TNF inhibitor therapy.</p>","PeriodicalId":9150,"journal":{"name":"BMC Rheumatology","volume":"9 1","pages":"39"},"PeriodicalIF":2.5000,"publicationDate":"2025-04-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11974236/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41927-025-00489-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: This study evaluates the long-term effectiveness and safety of methotrexate-tacrolimus combination therapy compared to methotrexate monotherapy in maintaining successful tumor necrosis factor (TNF) inhibitor discontinuation in rheumatoid arthritis (RA) patients.
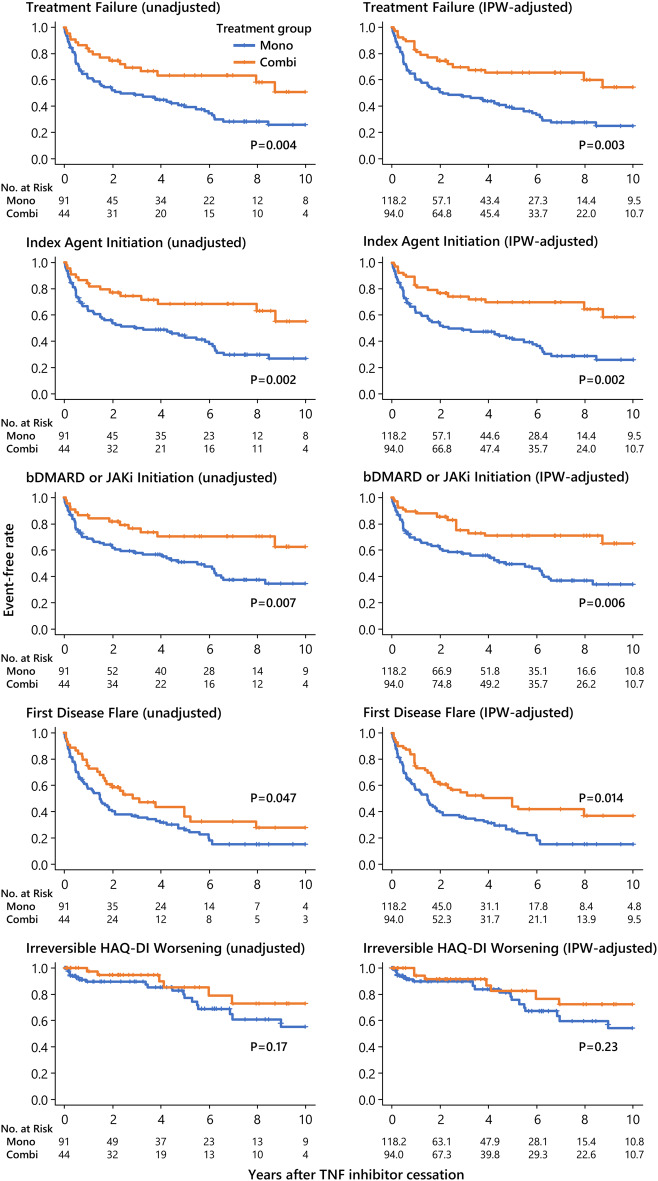
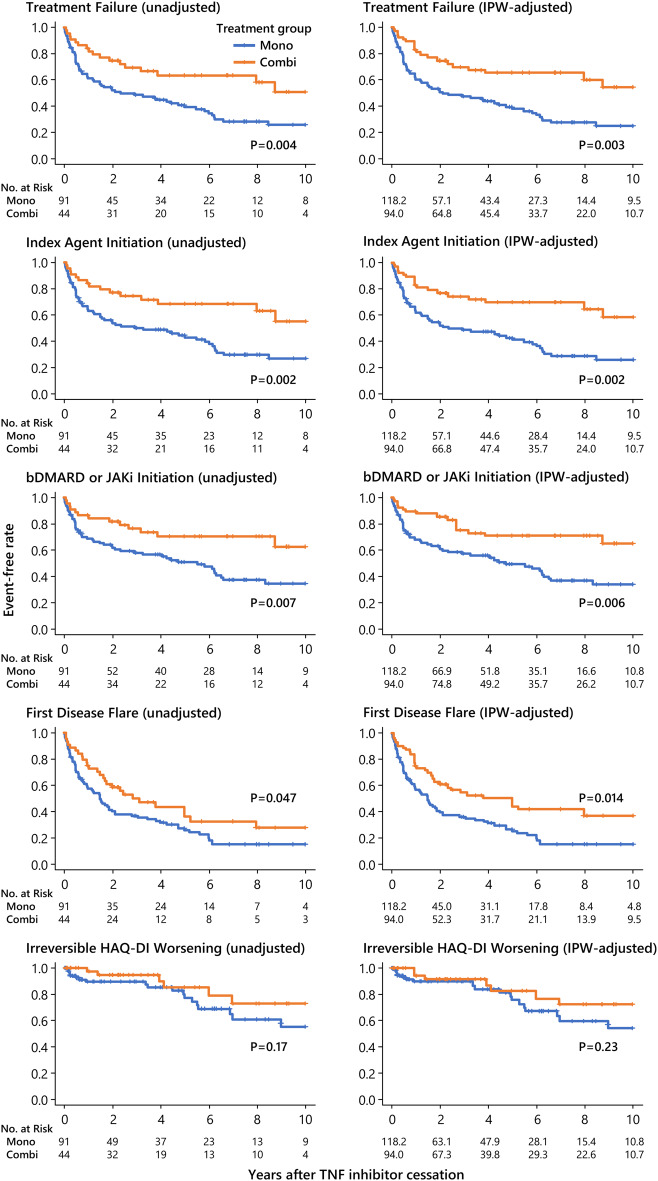
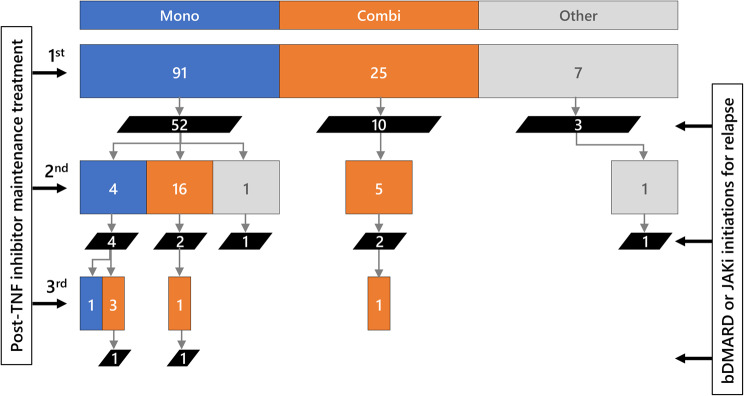
Methods: We retrospectively analyzed consecutive RA patients who discontinued TNF inhibitors after achieving disease control by October 2022 and received either methotrexate monotherapy or methotrexate-tacrolimus combination therapy for up to 10 years. Per-observation time-to-event analyses assessed treatment failure, treatment intensification, first disease flare, and irreversible functional deterioration. Mixed-effects Cox models, time-dependent Cox models without random effects, and Kaplan-Meier estimates with inverse probability weighting were applied. Safety assessment included treatment-limiting adverse events and renal function trends.
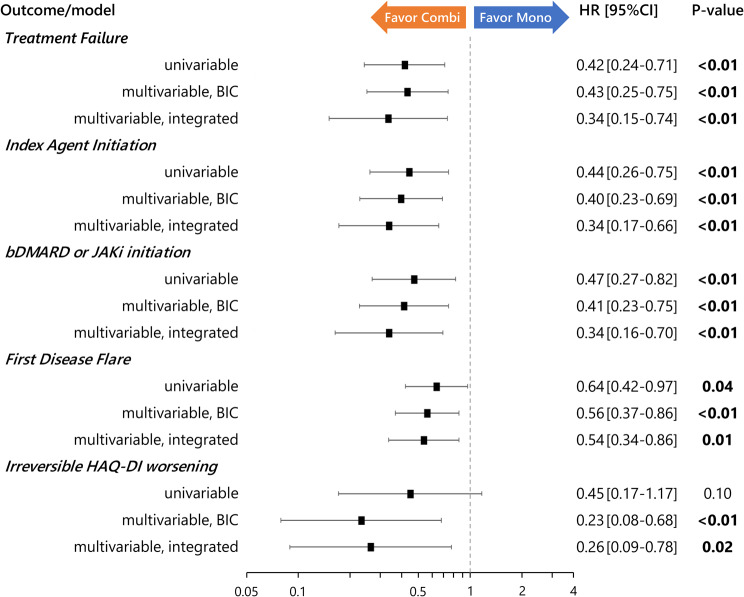
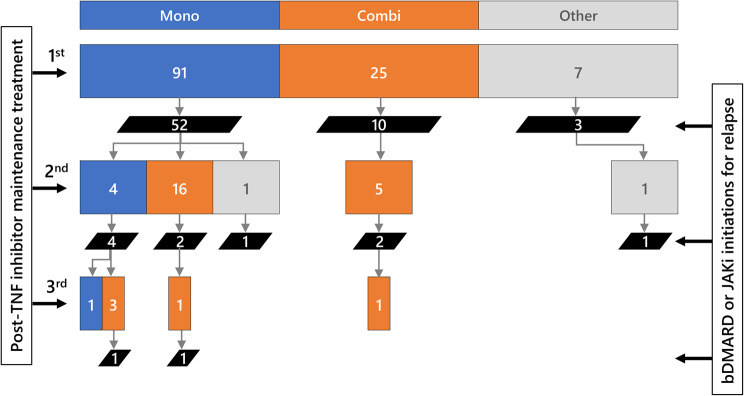
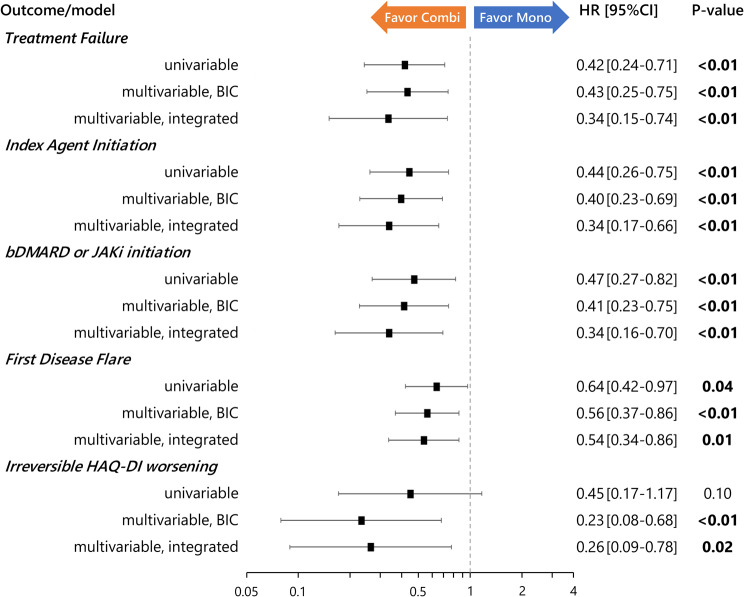
Results: A total of 147 treatment lines (96 methotrexate monotherapy and 51 combination therapy) in 116 patients were analyzed. The combination therapy significantly reduced treatment failure (hazard ratio [HR], 0.42; 95% confidence interval [CI], 0.24-0.72), treatment intensification with the index drugs (HR, 0.38; 95% CI, 0.22-0.67) and with biologics or Janus kinase inhibitors (HR, 0.39; 95% CI, 0.22-0.71), and first flare (HR, 0.55; 95%CI 0.36-0.84), with consistent findings across models. The benefit was most pronounced in patients with prior flares during methotrexate monotherapy after TNF inhibitor discontinuation, with HRs as low as 0.04-0.12 across outcomes. No significant differences in treatment-limiting adverse events were observed. The annual increase in serum creatinine for tacrolimus users was 0.0032 mg/dL, suggesting minimal long-term renal impact.
Conclusions: Methotrexate-tacrolimus combination therapy significantly reduces relapse risk following TNF inhibitor discontinuation without compromising safety, offering a potentially sustainable treatment alternative after achieving remission with TNF inhibitor therapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


