{"title":"Dynamic left ventricular outflow tract obstruction induced by intra-aortic balloon pump in patient with angioedema.","authors":"Konstantin Yastrebov, Gregory Cranney","doi":"10.1186/s13089-025-00426-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Intra-aortic balloon pump is used for temporary mechanical support of failing left ventricle. It works by reducing the arterial afterload during ventricular systole to reduce myocardial work and increasing diastolic proximal aortic pressure to improve coronary perfusion. Rarely, intra-aortic balloon pump (IABP) can become the cause of severe haemodynamic compromise, causing dynamic left ventricular outflow tract obstruction.</p><p><strong>Case presentation: </strong>An 88-yo man presented with angiotensin converting enzyme inhibitor (ACEI) - induced angioedema. He received steroids and adrenaline, but progressed to the respiratory arrest, requiring emergency awake fiberoptic intubation and mechanical ventilation. Echocardiography revealed catecholamine-induced reversed Takotsubo cardiomyopathy. The patient suffered asystolic cardiac arrest on arrival to intensive care unit (ICU), requiring cardiopulmonary resuscitation (CPR). Bradycardia and hypotension were treated with atrial pacing and (IABP). Icatibant was administered for angioedema. After several hours of haemodynamic stability, severe hypotension returned. Bedside echocardiographic diagnosis of recovery from Takotsubo and new development of IABP-induced dynamic left ventricular outflow tract obstruction (DLVOTO) was made. Stopping IABP resulted in rapid haemodynamic recovery. Repeated doses of Icatibant were needed. The patient survived and returned to independent living.</p><p><strong>Conclusions: </strong>Immediate echocardiographic recognition of iatrogenic DLVOTO caused by IABP allows discontinuation of IABP support as a life-saving intervention. Dynamic application of spectral Doppler with changes in IABP settings is required for correct diagnosis.</p>","PeriodicalId":36911,"journal":{"name":"Ultrasound Journal","volume":"17 1","pages":"22"},"PeriodicalIF":2.9000,"publicationDate":"2025-04-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11977056/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ultrasound Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-025-00426-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Intra-aortic balloon pump is used for temporary mechanical support of failing left ventricle. It works by reducing the arterial afterload during ventricular systole to reduce myocardial work and increasing diastolic proximal aortic pressure to improve coronary perfusion. Rarely, intra-aortic balloon pump (IABP) can become the cause of severe haemodynamic compromise, causing dynamic left ventricular outflow tract obstruction.
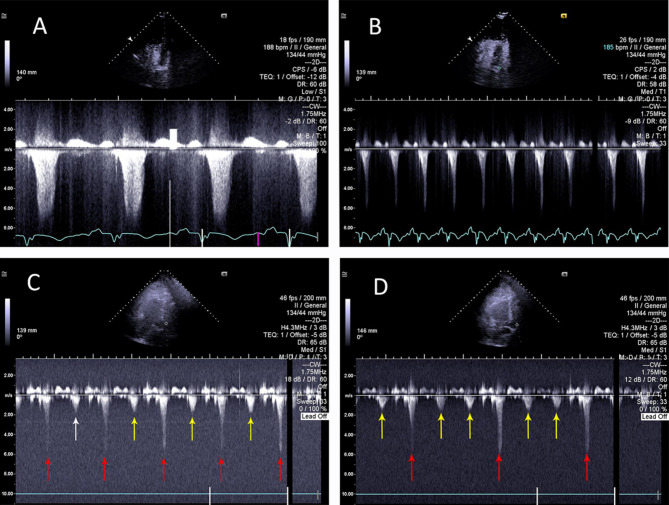
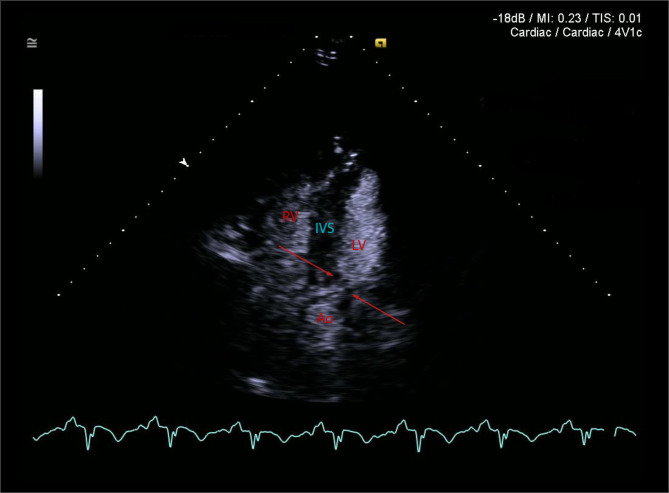
Case presentation: An 88-yo man presented with angiotensin converting enzyme inhibitor (ACEI) - induced angioedema. He received steroids and adrenaline, but progressed to the respiratory arrest, requiring emergency awake fiberoptic intubation and mechanical ventilation. Echocardiography revealed catecholamine-induced reversed Takotsubo cardiomyopathy. The patient suffered asystolic cardiac arrest on arrival to intensive care unit (ICU), requiring cardiopulmonary resuscitation (CPR). Bradycardia and hypotension were treated with atrial pacing and (IABP). Icatibant was administered for angioedema. After several hours of haemodynamic stability, severe hypotension returned. Bedside echocardiographic diagnosis of recovery from Takotsubo and new development of IABP-induced dynamic left ventricular outflow tract obstruction (DLVOTO) was made. Stopping IABP resulted in rapid haemodynamic recovery. Repeated doses of Icatibant were needed. The patient survived and returned to independent living.
Conclusions: Immediate echocardiographic recognition of iatrogenic DLVOTO caused by IABP allows discontinuation of IABP support as a life-saving intervention. Dynamic application of spectral Doppler with changes in IABP settings is required for correct diagnosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


