{"title":"Ambulance Service Utilization by Kidney Transplant Recipients.","authors":"Kaveh Masoumi-Ravandi, Amanda Vinson, Aran Thanamayooran, Judah Goldstein, Thomas Skinner, Karthik Tennankore","doi":"10.1177/20543581251324587","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Compared with the general population, kidney transplant recipients (KTRs) frequently visit the emergency department (ED), but much less is known about the characteristics of ED presentations requiring ambulance transport and the impact on subsequent outcomes for KTRs.</p><p><strong>Objectives: </strong>To identify predictors of ambulance transport to the ED (ambulance-ED) and outcomes (graft failure and mortality) for those who experienced an ambulance-ED event in a cohort of KTRs.</p><p><strong>Design: </strong>Retrospective cohort study of incident, adult KTRs receiving a transplant from 2008 to 2020.</p><p><strong>Setting: </strong>Nova Scotia, Canada.</p><p><strong>Patients: </strong>Adult (≥18 years), Nova Scotian KTRs affiliated with the Atlantic Canada Multi-Organ Transplant Program.</p><p><strong>Measurements: </strong>Ambulance-ED events were captured for all transplant recipients (following the day of discharge from their initial transplant admission) using electronic records (provided by Emergency Health Services, the sole provider of emergency medical services for Nova Scotia). Ambulance-ED was defined as ambulance transport to the ED following a 911 call; interfacility transfers were excluded. Predictors of ambulance-ED included recipient, donor, immunological, and perioperative characteristics (pertaining to the initial admission for kidney transplantation). Outcomes included graft failure and mortality.</p><p><strong>Methods: </strong>Predictors of ambulance-ED were analyzed using a multivariable negative binomial regression model and reported using incidence rate ratios (IRRs) and 95% confidence intervals (CIs). The risk of death/graft failure for those with an ambulance-ED within 30 days of hospital discharge following transplantation was analyzed using an adjusted Cox survival analysis and reported using hazard ratios (HRs) and 95% CIs.</p><p><strong>Results: </strong>A total of 418 patients received a transplant during the study period. A total of 179 (42.8%) experienced one or more ambulance-ED events. Female sex (IRR = 1.60; 95% CI = 1.12-2.29), kidney failure secondary to diabetes (IRR = 2.52; 95% CI = 1.19-5.31), and donor age ≥45 (IRR = 1.50; 95% CI = 1.04-2.15) were all associated with ambulance-ED. There was no significant increase in the risk of death/graft failure for those that experienced ambulance-ED within 30 days of hospital discharge following transplantation (HR = 1.31; 95% CI = 0.44-3.94).</p><p><strong>Limitations: </strong>A limitation of this study was that ambulance-ED is not a perfect surrogate marker of acute care needs in a population. Important determinants of health such as living situation and socioeconomic status were not available in this data set.</p><p><strong>Conclusions: </strong>This study highlights the burden of ambulance use for KTRs and provides insight into the need for more optimal follow-up in certain patient subgroups who are at particularly high risk.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"12 ","pages":"20543581251324587"},"PeriodicalIF":1.5000,"publicationDate":"2025-04-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11970094/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581251324587","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Compared with the general population, kidney transplant recipients (KTRs) frequently visit the emergency department (ED), but much less is known about the characteristics of ED presentations requiring ambulance transport and the impact on subsequent outcomes for KTRs.
Objectives: To identify predictors of ambulance transport to the ED (ambulance-ED) and outcomes (graft failure and mortality) for those who experienced an ambulance-ED event in a cohort of KTRs.
Design: Retrospective cohort study of incident, adult KTRs receiving a transplant from 2008 to 2020.
Setting: Nova Scotia, Canada.
Patients: Adult (≥18 years), Nova Scotian KTRs affiliated with the Atlantic Canada Multi-Organ Transplant Program.
Measurements: Ambulance-ED events were captured for all transplant recipients (following the day of discharge from their initial transplant admission) using electronic records (provided by Emergency Health Services, the sole provider of emergency medical services for Nova Scotia). Ambulance-ED was defined as ambulance transport to the ED following a 911 call; interfacility transfers were excluded. Predictors of ambulance-ED included recipient, donor, immunological, and perioperative characteristics (pertaining to the initial admission for kidney transplantation). Outcomes included graft failure and mortality.
Methods: Predictors of ambulance-ED were analyzed using a multivariable negative binomial regression model and reported using incidence rate ratios (IRRs) and 95% confidence intervals (CIs). The risk of death/graft failure for those with an ambulance-ED within 30 days of hospital discharge following transplantation was analyzed using an adjusted Cox survival analysis and reported using hazard ratios (HRs) and 95% CIs.
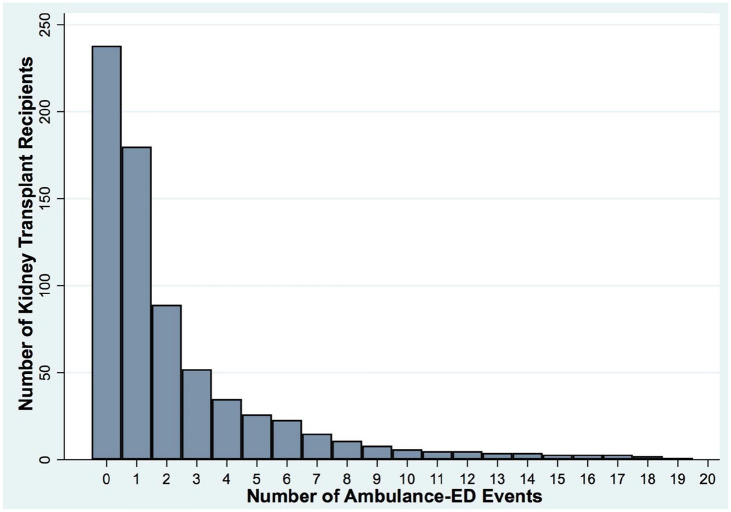
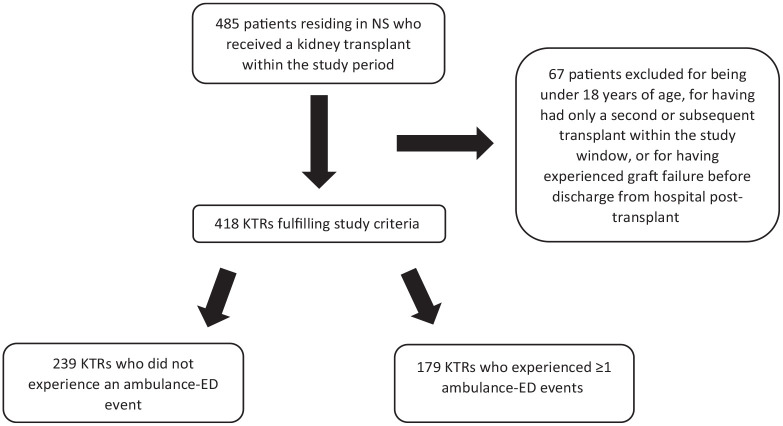
Results: A total of 418 patients received a transplant during the study period. A total of 179 (42.8%) experienced one or more ambulance-ED events. Female sex (IRR = 1.60; 95% CI = 1.12-2.29), kidney failure secondary to diabetes (IRR = 2.52; 95% CI = 1.19-5.31), and donor age ≥45 (IRR = 1.50; 95% CI = 1.04-2.15) were all associated with ambulance-ED. There was no significant increase in the risk of death/graft failure for those that experienced ambulance-ED within 30 days of hospital discharge following transplantation (HR = 1.31; 95% CI = 0.44-3.94).
Limitations: A limitation of this study was that ambulance-ED is not a perfect surrogate marker of acute care needs in a population. Important determinants of health such as living situation and socioeconomic status were not available in this data set.
Conclusions: This study highlights the burden of ambulance use for KTRs and provides insight into the need for more optimal follow-up in certain patient subgroups who are at particularly high risk.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


