The effect of expanded access to mental health care on economic status of households with a person with a mental disorder in rural Ethiopia: a controlled before-after study.
Yohannes Hailemichael, Damen Hailemariam, Kebede Tirfessa, Sumaiyah Docrat, Atalay Alem, Girmay Medhin, Abebaw Fekadu, Crick Lund, Dan Chisholm, Charlotte Hanlon
{"title":"The effect of expanded access to mental health care on economic status of households with a person with a mental disorder in rural Ethiopia: a controlled before-after study.","authors":"Yohannes Hailemichael, Damen Hailemariam, Kebede Tirfessa, Sumaiyah Docrat, Atalay Alem, Girmay Medhin, Abebaw Fekadu, Crick Lund, Dan Chisholm, Charlotte Hanlon","doi":"10.1186/s13033-025-00668-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Poverty and mental illness are strongly associated. The aim of this study was to investigate the economic impact of implementing a district level integrated mental healthcare plan for people with severe mental disorders (SMD) and depression compared to secular trends in the general population in a rural Ethiopian setting.</p><p><strong>Methods: </strong>A community-based, controlled before-after study design was used to assess changes in household economic status and catastrophic out-of-pocket (OOP) payments in relation to expanded access to mental health care. Two household samples were recruited, each with a community control group: (1) SMD sub-study and (2) depression sub-study. In the SMD sub-study, 290 households containing a member with SMD and 289 comparison households without a person with SMD participated. In the depression sub-study, 129 households with a person with depression and 129 comparison households. The case and comparison cohorts were followed up over 12 months. Propensity score matching and multivariable regression analyses were conducted.</p><p><strong>Results: </strong>Provision of mental healthcare in the district was associated with a greater increase in income (Birr 919.53, 95% CI: 34.49, 4573.56) but no significant changes in consumption expenditure (Birr 176.25, 95% CI: -1338.19, 1690.70) in households of people with SMD compared to secular trends in comparison households. In households of people with depression, there was no significant change in income (Birr 227.78, 95% CI: -1361.21, 1816.79) or consumption expenditure (Birr - 81.20, 95% CI: -2572.57, 2410.15). The proportion of households incurring catastrophic OOP health expenditure (COOPHE) at the ≥ 10% and ≥ 40% thresholds were significantly reduced after the intervention in the SMD (from 20.3 to 9.0%, p = 0.002, and 31.9-14.9%, p < 0.001) and in the depression intervention (from 19.6 to 5.3%, p = 0.003, and 25.2-11.8%, p = 0.015). Similarly, COOPHE has declined in the comparison households for SMD (from 15.6% (T1) to 8.2% (T2) (p = 0.035) and for depression comparison households (from12.1-4.1%(p = 0.069). However, there was no significant difference in the proportion of households experiencing catastrophic OOP health care expenditure in the SMD, depression and the comparison groups (p = 0.808 and p = 0.779 ). Despite improvement in income and COOPHE, households of persons with SMD or depression remained impoverished relative to comparison groups at follow-up. Households of people with SMD and depression were significantly less likely to be enrolled in community-based health insurance (CBHI) than comparison households.</p><p><strong>Conclusions: </strong>The District mental health care plan intervention increased household income and reduced catastrophic out-of- pocket payment. Our findings support global initiatives to scale up mental healthcare as part of universal health coverage initiatives, alongside interventions to support social inclusion and targeted financial protection for vulnerable households.</p>","PeriodicalId":47752,"journal":{"name":"International Journal of Mental Health Systems","volume":"19 1","pages":"12"},"PeriodicalIF":3.8000,"publicationDate":"2025-04-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11969764/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Mental Health Systems","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13033-025-00668-8","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PSYCHIATRY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Poverty and mental illness are strongly associated. The aim of this study was to investigate the economic impact of implementing a district level integrated mental healthcare plan for people with severe mental disorders (SMD) and depression compared to secular trends in the general population in a rural Ethiopian setting.
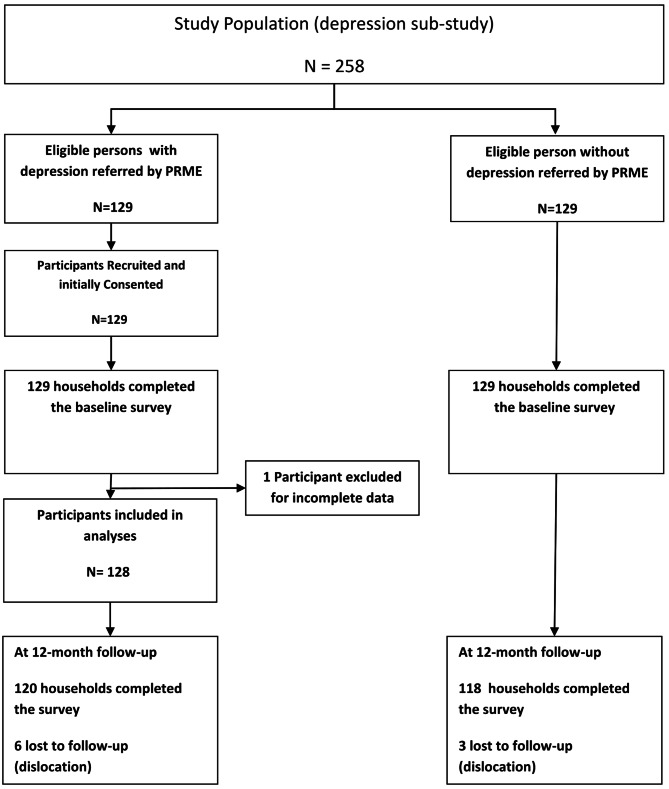
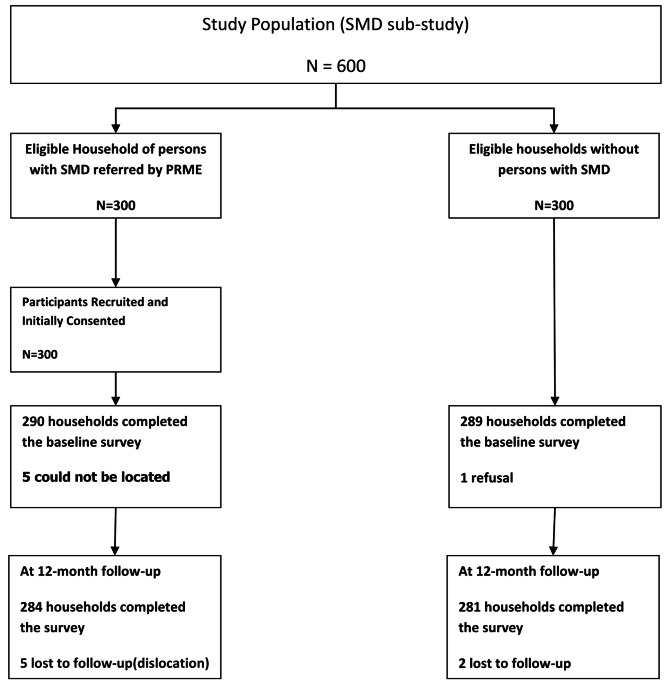
Methods: A community-based, controlled before-after study design was used to assess changes in household economic status and catastrophic out-of-pocket (OOP) payments in relation to expanded access to mental health care. Two household samples were recruited, each with a community control group: (1) SMD sub-study and (2) depression sub-study. In the SMD sub-study, 290 households containing a member with SMD and 289 comparison households without a person with SMD participated. In the depression sub-study, 129 households with a person with depression and 129 comparison households. The case and comparison cohorts were followed up over 12 months. Propensity score matching and multivariable regression analyses were conducted.
Results: Provision of mental healthcare in the district was associated with a greater increase in income (Birr 919.53, 95% CI: 34.49, 4573.56) but no significant changes in consumption expenditure (Birr 176.25, 95% CI: -1338.19, 1690.70) in households of people with SMD compared to secular trends in comparison households. In households of people with depression, there was no significant change in income (Birr 227.78, 95% CI: -1361.21, 1816.79) or consumption expenditure (Birr - 81.20, 95% CI: -2572.57, 2410.15). The proportion of households incurring catastrophic OOP health expenditure (COOPHE) at the ≥ 10% and ≥ 40% thresholds were significantly reduced after the intervention in the SMD (from 20.3 to 9.0%, p = 0.002, and 31.9-14.9%, p < 0.001) and in the depression intervention (from 19.6 to 5.3%, p = 0.003, and 25.2-11.8%, p = 0.015). Similarly, COOPHE has declined in the comparison households for SMD (from 15.6% (T1) to 8.2% (T2) (p = 0.035) and for depression comparison households (from12.1-4.1%(p = 0.069). However, there was no significant difference in the proportion of households experiencing catastrophic OOP health care expenditure in the SMD, depression and the comparison groups (p = 0.808 and p = 0.779 ). Despite improvement in income and COOPHE, households of persons with SMD or depression remained impoverished relative to comparison groups at follow-up. Households of people with SMD and depression were significantly less likely to be enrolled in community-based health insurance (CBHI) than comparison households.
Conclusions: The District mental health care plan intervention increased household income and reduced catastrophic out-of- pocket payment. Our findings support global initiatives to scale up mental healthcare as part of universal health coverage initiatives, alongside interventions to support social inclusion and targeted financial protection for vulnerable households.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


