Prognosis of low-flow low-gradient aortic valve stenosis with atrial fibrillation
IF 2.6
3区 医学
Q2 CARDIAC & CARDIOVASCULAR SYSTEMS
引用次数: 0
Abstract
Background
The prognosis for patients with low-flow low-gradient (LFLG) aortic valve stenosis (AS) remains controversial. In general, atrial fibrillation (AF) is one factor determining the LF status in patients with severe AS (SAS). However, the association between concomitant AF in LFLG AS and the risk of heart failure (HF) remains unclear.
Methods
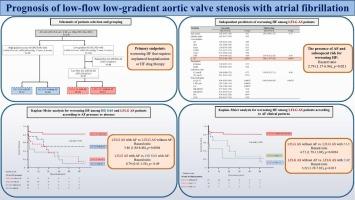
This study evaluated 278 consecutive patients with SAS (indexed aortic valve area < 0.6 cm2/m2). Among them, we enrolled patients with high-gradient (HG) SAS [mean pressure gradient (mPG) ≥40 mmHg] and LFLG AS (stroke volume index ≤35 ml/m2, mPG <40 mmHg). The two groups were further categorized into four subgroups following the presence or absence of AF as HG SAS with AF (n = 27), HG SAS without AF (n = 68), LFLG AS with AF (n = 30), and LFLG AS without AF (n = 67). The primary endpoint was worsening HF that required unplanned hospitalization or HF drug therapy.
Results
We observed worsening HF in 65 patients. The Kaplan–Meier curve revealed a higher rate of worsening HF in LFLG AS with AF than that in HG SAS without AF (log-rank p < 0.001) without any significant difference compared to HG SAS with AF. The Cox hazard analysis among LFLG AS patients identified the presence of AF as an independent predictor for worsening HF [hazard ratio (HR): 2.79; 95 % confidence interval (CI): 1.17–6.96; p = 0.021]. In addition, the Kaplan–Meier analysis curve revealed a higher risk of worsening HF in patients with LFLG AS and paroxysmal AF (PAF) or chronic AF (CAF) than in those without AF (PAF: HR: 4.71, 95 % CI: 1.79–11.9, p = 0.0024; CAF: HR: 3.22, 95 % CI: 1.29–7.83, p = 0.013, respectively).
Conclusions
Patients with LFLG AS and concomitant AF exhibited an unfavorable prognosis for HF, with no significantly different rate of worsening HF compared with patients with HG SAS and conc.
低流量低梯度主动脉瓣狭窄合并心房颤动的预后。
背景:低流量低梯度(LFLG)主动脉瓣狭窄(AS)患者的预后仍有争议。一般来说,心房颤动(AF)是决定严重AS (SAS)患者LF状态的因素之一。然而,LFLG AS合并房颤与心力衰竭(HF)风险之间的关系尚不清楚。方法:本研究评估278例SAS(主动脉瓣指数面积 2/m2)患者。其中,我们纳入了高梯度(HG) SAS[平均压力梯度(mPG)≥40 mmHg]和LFLG AS(脑卒中容积指数≤35 ml/m2, mPG)患者。结果:65例患者HF恶化。Kaplan-Meier曲线显示,LFLG AS合并房颤的HF恶化率高于不合并房颤的HG SAS (log-rank p )。结论:LFLG AS合并房颤的患者HF预后不良,与HG SAS合并房颤的患者相比,HF恶化率无显著差异。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊
Journal of cardiology
CARDIAC & CARDIOVASCULAR SYSTEMS-
CiteScore
4.90
自引率
8.00%
发文量
202
审稿时长
29 days
期刊介绍:
The official journal of the Japanese College of Cardiology is an international, English language, peer-reviewed journal publishing the latest findings in cardiovascular medicine. Journal of Cardiology (JC) aims to publish the highest-quality material covering original basic and clinical research on all aspects of cardiovascular disease. Topics covered include ischemic heart disease, cardiomyopathy, valvular heart disease, vascular disease, hypertension, arrhythmia, congenital heart disease, pharmacological and non-pharmacological treatment, new diagnostic techniques, and cardiovascular imaging. JC also publishes a selection of review articles, clinical trials, short communications, and important messages and letters to the editor.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


