Shriram Swaminathan, Nithya Neelakantan, Henry Bryant, Pimvara Rattanamastip, Gagandeep Sandhu, Bobby Chacko
{"title":"Characterisation of IgA Nephropathy in an Australian Cohort.","authors":"Shriram Swaminathan, Nithya Neelakantan, Henry Bryant, Pimvara Rattanamastip, Gagandeep Sandhu, Bobby Chacko","doi":"10.1155/ijne/9976879","DOIUrl":null,"url":null,"abstract":"<p><p><b>Aim:</b> This retrospective cohort study aims to evaluate the prognostic factors for progression of immunoglobulin A nephropathy (IgAN) to kidney failure (defined as the initiation of kidney replacement therapy or death) and all-cause mortality in an Australian population. <b>Methods:</b> We conducted a retrospective analysis of 363 individual patients with biopsy-proven IgAN over a 21-year period (2000-2020) in the Hunter Region of New South Wales. Demographic data, comorbidities, biopsy features and biochemical markers were collected for a minimum of 12 months following biopsy diagnosis. A multivariable analysis using Cox regression was performed to examine their association with renal progression. <b>Results:</b> A total of 104 patients met the inclusion criteria and were followed for a median of 72 months. The cohort had a mean age at presentation of 45 years, with a predominantly male population. Most patients presented with haematuria and non-nephrotic range proteinuria. We stratified patients into three risk categories: low risk, intermediate risk, and high risk. Twenty-eight patients (26.92%) developed kidney failure and 15 patients (14.4%) experienced a > 20 mL/min eGFR decline within the first 12 months. The multivariable analysis revealed the following key factors associated with kidney failure: additional renal pathology on biopsy (HR 3.90, 95% CI 1.63-9.29), proteinuria (HR 1.15, 95% CI 1.02-1.29) and moderate-severe interstitial fibrosis/tubular atrophy (T2) (HR 7.00, 95% CI 2.32-21.05). There were 17 deaths (16.3%) in the cohort, with a mean survival time of 167.8 months (95% CI 152.6-183.1). <b>Conclusion:</b> In contrast to earlier reports from Australia, our findings emphasise that the progression to kidney failure is not uncommon in IgAN. We identified several predictors of the renal progression that are consistent with the previous studies. This highlights the need for a change in clinical management, as IgAN should no longer be considered a benign condition.</p>","PeriodicalId":14177,"journal":{"name":"International Journal of Nephrology","volume":"2025 ","pages":"9976879"},"PeriodicalIF":1.4000,"publicationDate":"2025-03-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11968155/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/ijne/9976879","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
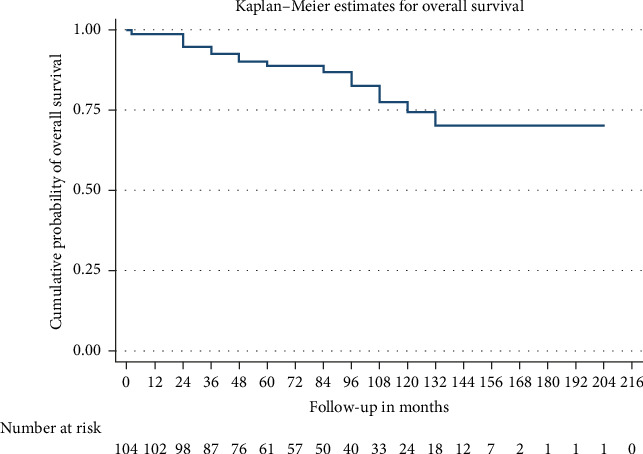
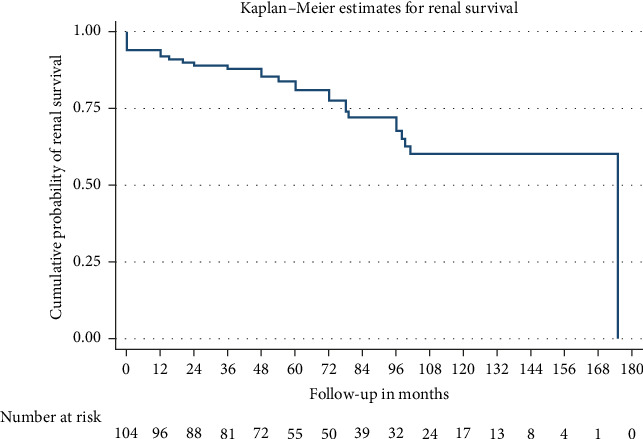
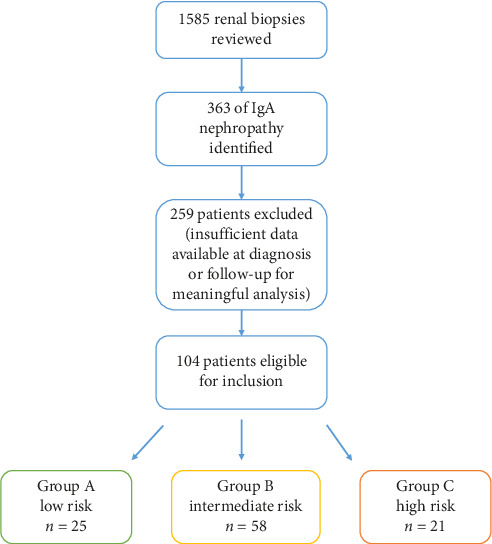
Aim: This retrospective cohort study aims to evaluate the prognostic factors for progression of immunoglobulin A nephropathy (IgAN) to kidney failure (defined as the initiation of kidney replacement therapy or death) and all-cause mortality in an Australian population. Methods: We conducted a retrospective analysis of 363 individual patients with biopsy-proven IgAN over a 21-year period (2000-2020) in the Hunter Region of New South Wales. Demographic data, comorbidities, biopsy features and biochemical markers were collected for a minimum of 12 months following biopsy diagnosis. A multivariable analysis using Cox regression was performed to examine their association with renal progression. Results: A total of 104 patients met the inclusion criteria and were followed for a median of 72 months. The cohort had a mean age at presentation of 45 years, with a predominantly male population. Most patients presented with haematuria and non-nephrotic range proteinuria. We stratified patients into three risk categories: low risk, intermediate risk, and high risk. Twenty-eight patients (26.92%) developed kidney failure and 15 patients (14.4%) experienced a > 20 mL/min eGFR decline within the first 12 months. The multivariable analysis revealed the following key factors associated with kidney failure: additional renal pathology on biopsy (HR 3.90, 95% CI 1.63-9.29), proteinuria (HR 1.15, 95% CI 1.02-1.29) and moderate-severe interstitial fibrosis/tubular atrophy (T2) (HR 7.00, 95% CI 2.32-21.05). There were 17 deaths (16.3%) in the cohort, with a mean survival time of 167.8 months (95% CI 152.6-183.1). Conclusion: In contrast to earlier reports from Australia, our findings emphasise that the progression to kidney failure is not uncommon in IgAN. We identified several predictors of the renal progression that are consistent with the previous studies. This highlights the need for a change in clinical management, as IgAN should no longer be considered a benign condition.
期刊介绍:
International Journal of Nephrology is a peer-reviewed, Open Access journal that publishes original research articles, review articles, and clinical studies focusing on the prevention, diagnosis, and management of kidney diseases and associated disorders. The journal welcomes submissions related to cell biology, developmental biology, genetics, immunology, pathology, pathophysiology of renal disease and progression, clinical nephrology, dialysis, and transplantation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


