Salivary periostin levels as a non-invasive biomarker and their clinical correlates among healthy and periodontitis patients-a cross-sectional analytical study.
{"title":"Salivary periostin levels as a non-invasive biomarker and their clinical correlates among healthy and periodontitis patients-a cross-sectional analytical study.","authors":"Priyanka Padalkar, Sunaina Shetty Yadadi, Gopinath Vivekanandan, Shishir Ram Shetty, Mangesh Andhare, Aditi Pashine, Vineet Vinay, Vijay Desai, Raghavendra M Shetty","doi":"10.3389/fdmed.2025.1512252","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The diagnosis of periodontitis is primarily through clinical and radiographic assessments. However, it is difficult for clinicians to detect incipient periodontitis during the routine clinical assessment. Identifying people at risk for periodontitis and tracking disease development need a dependable biomarker. Currently, no biomarkers meet all the criteria required for an ideal diagnostic test. Therefore, the clinical utility of salivary periostin as a potential screening tool for periodontitis warrants further investigation, particularly through large samples across diverse populations. The present study aimed to investigate salivary periostin levels as a biomarker in individuals with periodontitis and healthy controls.</p><p><strong>Methods: </strong>Forty-five patients with generalized periodontitis stage III grade A/B and an equivalent number of periodontally healthy controls were evaluated for plaque index (PI), gingival index (GI), pocket probing depth (PPD), and clinical attachment level (CAL). Unstimulated salivary samples from all subjects were taken, and periostin levels were quantified using an ELISA kit.</p><p><strong>Results: </strong>The average salivary periostin levels were 4.63 in the healthy group and 1.24 in the periodontitis group (<i>P</i> < 0.05). The Spearman coefficient indicated a negative correlation between periostin levels and the gingival index (<i>r</i> = -0.761), plaque index (<i>r</i> = -0.780; <i>P</i> < 0.05), probing pocket depth (PPD) (<i>r</i> = -0.713; <i>P</i> < 0.05) and clinical attachment level (CAL) (<i>r</i> = -0.713; <i>P</i> < 0.05). Linear regression analysis validated the indirect correlation between salivary periostin levels and clinical indicators (Adjusted R square = 0.947).</p><p><strong>Conclusions: </strong>Salivary periostin levels are associated with periodontal disease. Salivary periostin levels indirectly influence as a non-invasive biomarker of periodontitis. The biomarker periostin is effective for evaluating both healthy and diseased periodontium.</p>","PeriodicalId":73077,"journal":{"name":"Frontiers in dental medicine","volume":"6 ","pages":"1512252"},"PeriodicalIF":1.8000,"publicationDate":"2025-03-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11961936/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in dental medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fdmed.2025.1512252","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"DENTISTRY, ORAL SURGERY & MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The diagnosis of periodontitis is primarily through clinical and radiographic assessments. However, it is difficult for clinicians to detect incipient periodontitis during the routine clinical assessment. Identifying people at risk for periodontitis and tracking disease development need a dependable biomarker. Currently, no biomarkers meet all the criteria required for an ideal diagnostic test. Therefore, the clinical utility of salivary periostin as a potential screening tool for periodontitis warrants further investigation, particularly through large samples across diverse populations. The present study aimed to investigate salivary periostin levels as a biomarker in individuals with periodontitis and healthy controls.
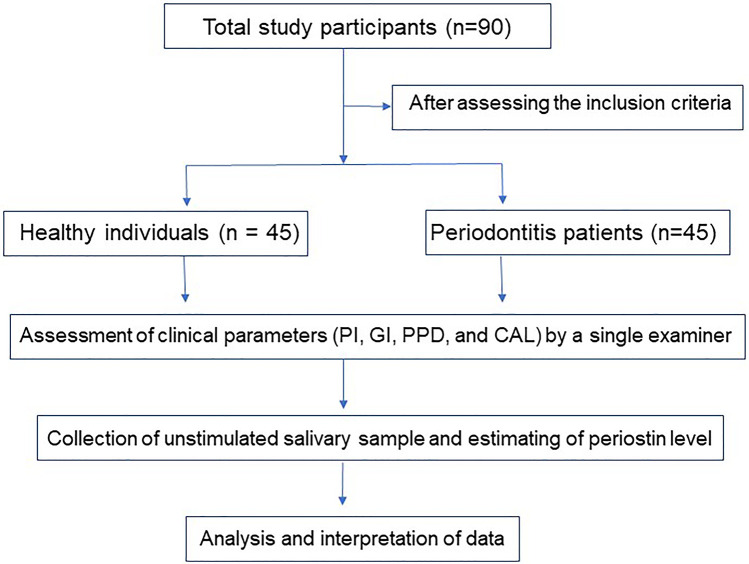
Methods: Forty-five patients with generalized periodontitis stage III grade A/B and an equivalent number of periodontally healthy controls were evaluated for plaque index (PI), gingival index (GI), pocket probing depth (PPD), and clinical attachment level (CAL). Unstimulated salivary samples from all subjects were taken, and periostin levels were quantified using an ELISA kit.
Results: The average salivary periostin levels were 4.63 in the healthy group and 1.24 in the periodontitis group (P < 0.05). The Spearman coefficient indicated a negative correlation between periostin levels and the gingival index (r = -0.761), plaque index (r = -0.780; P < 0.05), probing pocket depth (PPD) (r = -0.713; P < 0.05) and clinical attachment level (CAL) (r = -0.713; P < 0.05). Linear regression analysis validated the indirect correlation between salivary periostin levels and clinical indicators (Adjusted R square = 0.947).
Conclusions: Salivary periostin levels are associated with periodontal disease. Salivary periostin levels indirectly influence as a non-invasive biomarker of periodontitis. The biomarker periostin is effective for evaluating both healthy and diseased periodontium.
背景:牙周炎的诊断主要是通过临床和放射学评估。然而,临床医生在常规临床评估中很难发现早期牙周炎。识别有牙周炎风险的人群和追踪疾病发展需要一种可靠的生物标志物。目前,没有生物标记物满足理想诊断测试所需的所有标准。因此,唾液骨膜素作为牙周炎潜在筛查工具的临床应用值得进一步研究,特别是通过不同人群的大样本。本研究旨在探讨唾液骨膜蛋白水平作为牙周炎患者和健康对照者的生物标志物。方法:对45例广泛性牙周炎III期A/B级患者和同等数量的牙周健康对照者进行菌斑指数(PI)、牙龈指数(GI)、牙袋探诊深度(PPD)和临床依恋水平(CAL)的评估。采集所有受试者未受刺激的唾液样本,使用ELISA试剂盒定量测定骨膜素水平。结果:正常组和牙周炎组唾液骨膜素平均水平分别为4.63和1.24 (P r = -0.761),菌斑指数(r = -0.780;P r = -0.713;P r = -0.713;结论:唾液骨膜素水平与牙周病相关。唾液骨膜素水平作为一种非侵入性生物标志物间接影响牙周炎。生物标志物骨膜素是有效的评估健康和患病牙周组织。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


