{"title":"Impact of health intervention coverage on reducing maternal mortality in 126 low- and middle-income countries: a Lives Saved Tool modelling study.","authors":"Xi-Ru Guo, Jue Liu, Hai-Jun Wang","doi":"10.1186/s41256-025-00414-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There is a continued and urgent need to address the stagnation of the global maternal mortality ratio (MMR), especially for low- and middle-income countries (LMICs). We aimed to assess the impact of scaling up health intervention coverage on reducing MMR under four scenarios for 126 LMICs.</p><p><strong>Methods: </strong>We conducted the modelling study to estimate MMR and additional maternal lives saved by intervention by 2030 for 126 LMICs using the Lives Saved Tool (LiST). We applied four scenarios to assess the impact of scaling up health intervention coverage with no scale-up (no change), a modest scale-up (increased by 2% per year), a substantial scale-up (increased by 5% per year), and universal coverage (coverage reached 95% by 2030). In sensitivity analysis, with the current trend, we assumed that coverage of each intervention remained unchanged from 2024, with MMR changing according to the annual percentage change (APC) of 2015-2020.</p><p><strong>Results: </strong>Among the 126 LMICs, 31.7% (40/126) countries showed an increase in MMR, and 38.1% (48/126) stalled on the reduction of MMR from 2015 to 2020. With a modest, substantial, or universal scale-up, the 2030 average MMR would be 172.1 (117.6-262.9), 139.8 (95.6-213.5) or 98.6 (67.8-149.7), not reaching the SDG Target 3.1. Additional maternal lives saved by scaling up the coverage of health interventions were mainly clustered in the African Region, the Southeast Asia Region, and the Eastern Mediterranean Region. Compared with other included interventions, uterotonics for postpartum hemorrhage, assisted vaginal delivery and cesarean delivery played more important roles in reducing maternal mortality.</p><p><strong>Conclusions: </strong>The study findings highlighted that even under a substantial scale-up of intervention coverage or scaling up to universal coverage of interventions, it would be difficult for the 126 LMICs to achieve the SDG Target 3.1 on time. Optimizing the allocation of health resources, promoting health equality, taking more decisive national, regional and global actions are urgently needed for LMICs to reduce MMR and reach the SDG Target 3.1.</p>","PeriodicalId":52405,"journal":{"name":"Global Health Research and Policy","volume":"10 1","pages":"15"},"PeriodicalIF":4.6000,"publicationDate":"2025-04-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11963500/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Health Research and Policy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s41256-025-00414-0","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Background: There is a continued and urgent need to address the stagnation of the global maternal mortality ratio (MMR), especially for low- and middle-income countries (LMICs). We aimed to assess the impact of scaling up health intervention coverage on reducing MMR under four scenarios for 126 LMICs.
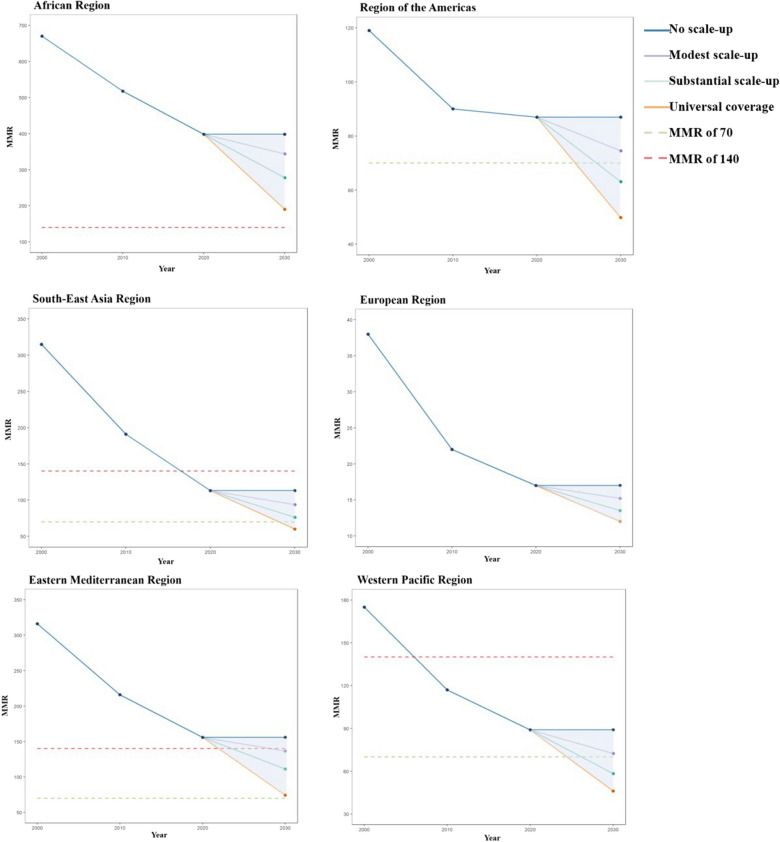
Methods: We conducted the modelling study to estimate MMR and additional maternal lives saved by intervention by 2030 for 126 LMICs using the Lives Saved Tool (LiST). We applied four scenarios to assess the impact of scaling up health intervention coverage with no scale-up (no change), a modest scale-up (increased by 2% per year), a substantial scale-up (increased by 5% per year), and universal coverage (coverage reached 95% by 2030). In sensitivity analysis, with the current trend, we assumed that coverage of each intervention remained unchanged from 2024, with MMR changing according to the annual percentage change (APC) of 2015-2020.
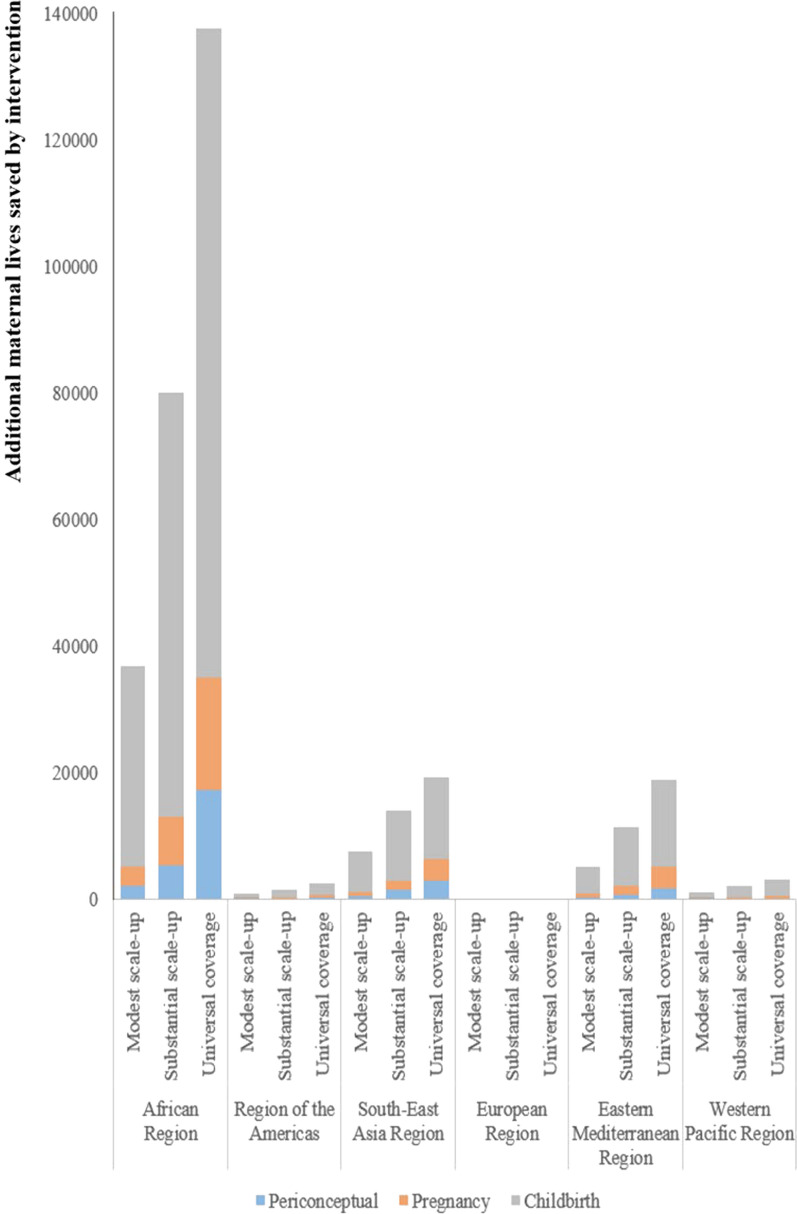
Results: Among the 126 LMICs, 31.7% (40/126) countries showed an increase in MMR, and 38.1% (48/126) stalled on the reduction of MMR from 2015 to 2020. With a modest, substantial, or universal scale-up, the 2030 average MMR would be 172.1 (117.6-262.9), 139.8 (95.6-213.5) or 98.6 (67.8-149.7), not reaching the SDG Target 3.1. Additional maternal lives saved by scaling up the coverage of health interventions were mainly clustered in the African Region, the Southeast Asia Region, and the Eastern Mediterranean Region. Compared with other included interventions, uterotonics for postpartum hemorrhage, assisted vaginal delivery and cesarean delivery played more important roles in reducing maternal mortality.
Conclusions: The study findings highlighted that even under a substantial scale-up of intervention coverage or scaling up to universal coverage of interventions, it would be difficult for the 126 LMICs to achieve the SDG Target 3.1 on time. Optimizing the allocation of health resources, promoting health equality, taking more decisive national, regional and global actions are urgently needed for LMICs to reduce MMR and reach the SDG Target 3.1.
期刊介绍:
Global Health Research and Policy, an open-access, multidisciplinary journal, publishes research on various aspects of global health, addressing topics like health equity, health systems and policy, social determinants of health, disease burden, population health, and other urgent global health issues. It serves as a forum for high-quality research focused on regional and global health improvement, emphasizing solutions for health equity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


