Left bundle branch area pacing prevails over His bundle pacing for heart failure patients undergoing atrioventricular node ablation in permanent atrial fibrillation: a network meta-analysis.
{"title":"Left bundle branch area pacing prevails over His bundle pacing for heart failure patients undergoing atrioventricular node ablation in permanent atrial fibrillation: a network meta-analysis.","authors":"Jing-Wen Ding, Yu-Ang Jiang, Qiu-Ting Wang, Chu Guo, Jian-Hui Yao, Gong-Qiang Dai, Jing-Chen, Huai-Sheng Ding","doi":"10.1007/s10840-025-02034-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Atrioventricular node ablation (AVNA) and pacemaker implantation enhance prognosis in heart failure patients experiencing rapid ventricular response due to atrial fibrillation. This meta-analysis assessed the clinical benefits of various pacing modalities following AVNA.</p><p><strong>Methods: </strong>The electrophysiological endpoint was defined as QRS duration, while the echocardiographic endpoint was the change in left ventricular ejection fraction. Secondary endpoints included pacing threshold, mortality rates, and improvements in the 6-min walk test.</p><p><strong>Results: </strong>This meta-analysis of 13 studies involving 1257 patients suggested that His bundle pacing (HBP) and left bundle branch area pacing (LBBAP) conferred an advantage in narrowing QRS duration compared to biventricular pacing (BVP) (HBP vs BVP OR = - 59.05, 95%CI = - 73.12 to - 44.97; LBBAP vs BVP OR = - 48.64, 95%CI = - 64.05 to - 33.24). The findings of echocardiographic endpoints suggested that LBBAP and HBP emerged as the optimal strategies over RVP (vs HBP OR = - 7.59, 95%CI = - 11.85 to - 3.32; vs LBBAP OR = - 6.58, 95%CI = - 12.08 to - 1.07). LBBAP reduced all-cause mortality compared to BVP (OR = 0.10, 95%CI = 0.01-0.78); however, no significant differences in all-cause mortality were observed between LBBAP and HBP. The pacing threshold of LBBAP was significantly lower than HBP (OR = - 0.40, 95%CI = - 0.57 to - 0.23).</p><p><strong>Conclusion: </strong>LBBAP not only demonstrated superior clinical outcomes regarding mortality compared to ventricular pacing strategies, but also was associated with a lower pacing threshold than HBP, thereby indicating its potential advantage over HBP in patients undergoing AVNA and subsequent pacemaker implantation.</p>","PeriodicalId":16202,"journal":{"name":"Journal of Interventional Cardiac Electrophysiology","volume":" ","pages":"1363-1372"},"PeriodicalIF":2.6000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12399726/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Interventional Cardiac Electrophysiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10840-025-02034-7","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/3 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Atrioventricular node ablation (AVNA) and pacemaker implantation enhance prognosis in heart failure patients experiencing rapid ventricular response due to atrial fibrillation. This meta-analysis assessed the clinical benefits of various pacing modalities following AVNA.
Methods: The electrophysiological endpoint was defined as QRS duration, while the echocardiographic endpoint was the change in left ventricular ejection fraction. Secondary endpoints included pacing threshold, mortality rates, and improvements in the 6-min walk test.
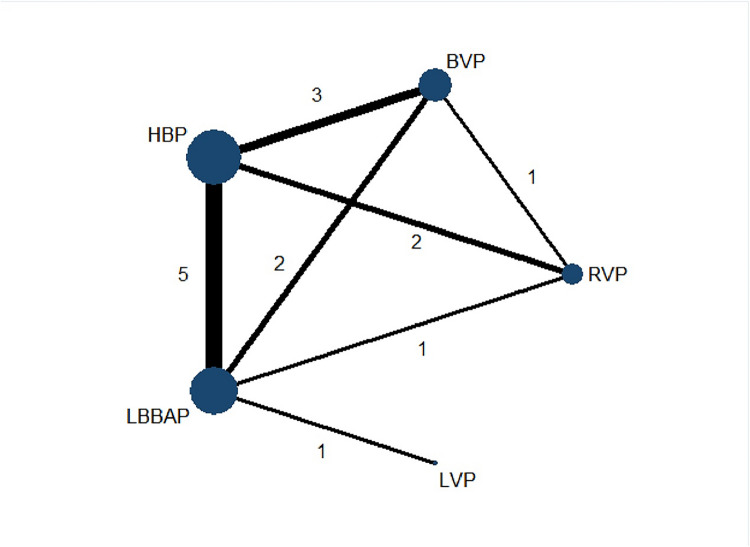
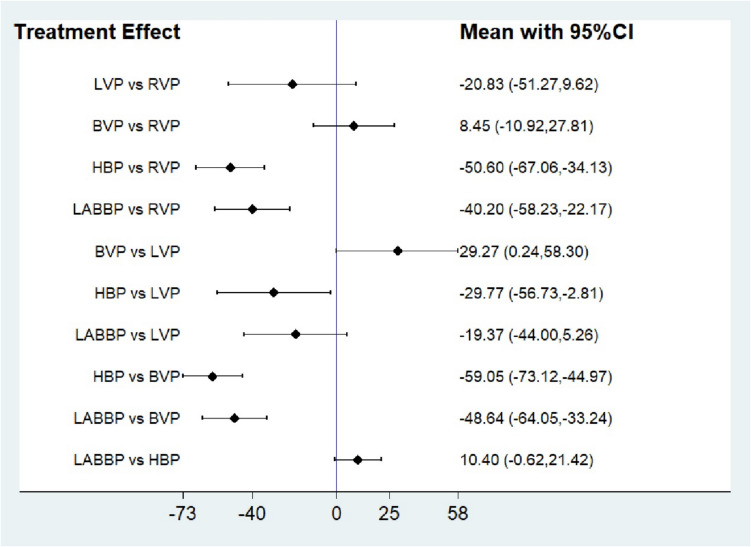
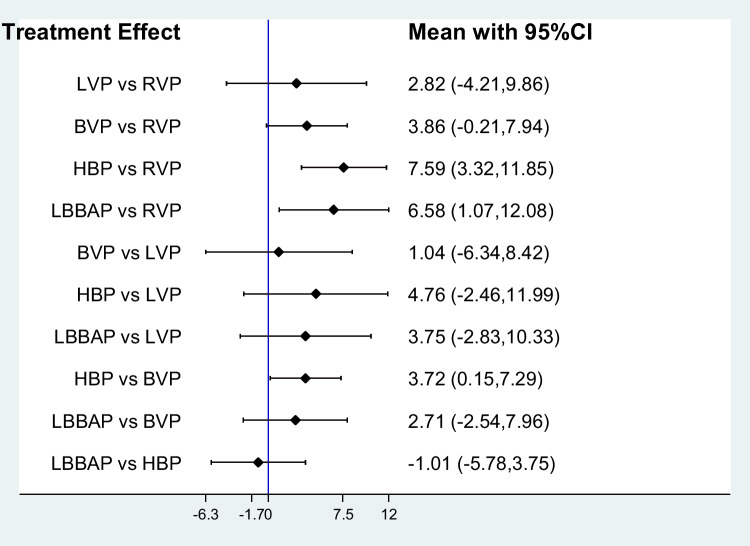
Results: This meta-analysis of 13 studies involving 1257 patients suggested that His bundle pacing (HBP) and left bundle branch area pacing (LBBAP) conferred an advantage in narrowing QRS duration compared to biventricular pacing (BVP) (HBP vs BVP OR = - 59.05, 95%CI = - 73.12 to - 44.97; LBBAP vs BVP OR = - 48.64, 95%CI = - 64.05 to - 33.24). The findings of echocardiographic endpoints suggested that LBBAP and HBP emerged as the optimal strategies over RVP (vs HBP OR = - 7.59, 95%CI = - 11.85 to - 3.32; vs LBBAP OR = - 6.58, 95%CI = - 12.08 to - 1.07). LBBAP reduced all-cause mortality compared to BVP (OR = 0.10, 95%CI = 0.01-0.78); however, no significant differences in all-cause mortality were observed between LBBAP and HBP. The pacing threshold of LBBAP was significantly lower than HBP (OR = - 0.40, 95%CI = - 0.57 to - 0.23).
Conclusion: LBBAP not only demonstrated superior clinical outcomes regarding mortality compared to ventricular pacing strategies, but also was associated with a lower pacing threshold than HBP, thereby indicating its potential advantage over HBP in patients undergoing AVNA and subsequent pacemaker implantation.
期刊介绍:
The Journal of Interventional Cardiac Electrophysiology is an international publication devoted to fostering research in and development of interventional techniques and therapies for the management of cardiac arrhythmias. It is designed primarily to present original research studies and scholarly scientific reviews of basic and applied science and clinical research in this field. The Journal will adopt a multidisciplinary approach to link physical, experimental, and clinical sciences as applied to the development of and practice in interventional electrophysiology. The Journal will examine techniques ranging from molecular, chemical and pharmacologic therapies to device and ablation technology. Accordingly, original research in clinical, epidemiologic and basic science arenas will be considered for publication. Applied engineering or physical science studies pertaining to interventional electrophysiology will be encouraged. The Journal is committed to providing comprehensive and detailed treatment of major interventional therapies and innovative techniques in a structured and clinically relevant manner. It is directed at clinical practitioners and investigators in the rapidly growing field of interventional electrophysiology. The editorial staff and board reflect this bias and include noted international experts in this area with a wealth of expertise in basic and clinical investigation. Peer review of all submissions, conflict of interest guidelines and periodic editorial board review of all Journal policies have been established.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


