{"title":"Endoscopic Ultrasound-Guided Fine-Needle Aspiration of Suspected Locoregional Rectal Cancer Localizations: A Valuable Tool.","authors":"Frank Ter Borg, Shira H de Bie, A Koen Talsma","doi":"10.1159/000544767","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Organ-preserving treatment for rectal cancer using local excision (LE) and/or chemoradiotherapy (CRT) is increasingly used. Locoregional metastasis precludes LE and locoregional regrowth, recurrence, or persistence after LE or chemoradiation (CRT) may prompt total mesorectal excision (TME). We believe that the time has passed to make such life-changing treatment decisions without pathological confirmation and investigated the use of linear endoscopic ultrasound with fine-needle aspiration (EUS-FNA).</p><p><strong>Case presentations: </strong>We report 8 cases of suspected locoregional tumor growth (LRTG) on MRI: adjacent or in the rectal wall, within the mesorectal fascia, high presacral region, and obturator foramen. MRI images were studied thoroughly before and during EUS to identify the target lesion using rectal EUS-FNA. Patients were prepared using an enema. The procedure was performed on an outpatient basis without conscious sedation. FNA was performed using a 25G needle. The patient received a 3-day course of ciprofloxacin after the procedure to prevent infection of the perirectal space. Identification of the target was the most difficult part of EUS but was successful in all cases. FNA revealed adenocarcinoma in 7 cases. Five cases were confirmed by TME results: 1 patient died before the operation, and 1 patient was treated with CRT. One patient with a suspected node in the obturator foramen was free of tumors on FNA. The TME resection specimen contained 31 lymph nodes without metastasis. All procedures were well tolerated, and no complications were observed.</p><p><strong>Conclusion: </strong>Suspected LRTG on MRI can be confirmed using EUS-FNA. In the era of organ-preserving treatment for rectal cancer, EUS-FNA may play a supportive role when considering TME or CRT.</p>","PeriodicalId":9614,"journal":{"name":"Case Reports in Gastroenterology","volume":"19 1","pages":"253-261"},"PeriodicalIF":0.6000,"publicationDate":"2025-04-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11964411/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000544767","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Organ-preserving treatment for rectal cancer using local excision (LE) and/or chemoradiotherapy (CRT) is increasingly used. Locoregional metastasis precludes LE and locoregional regrowth, recurrence, or persistence after LE or chemoradiation (CRT) may prompt total mesorectal excision (TME). We believe that the time has passed to make such life-changing treatment decisions without pathological confirmation and investigated the use of linear endoscopic ultrasound with fine-needle aspiration (EUS-FNA).
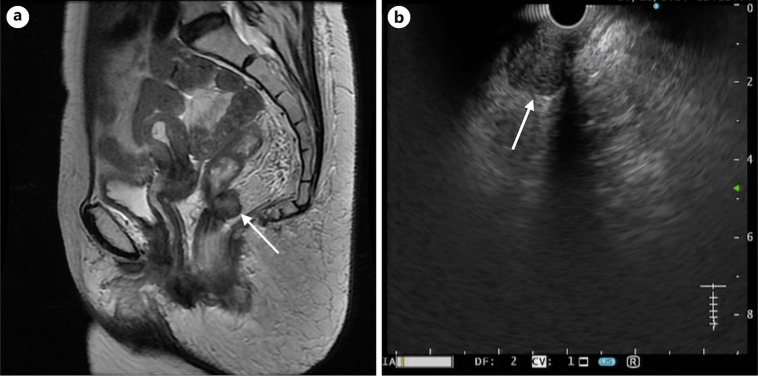
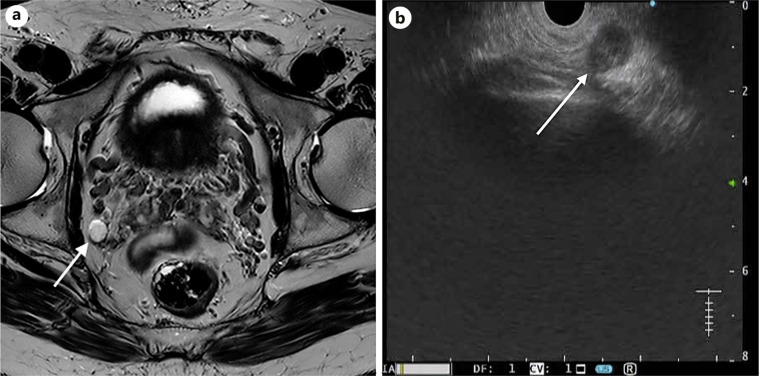
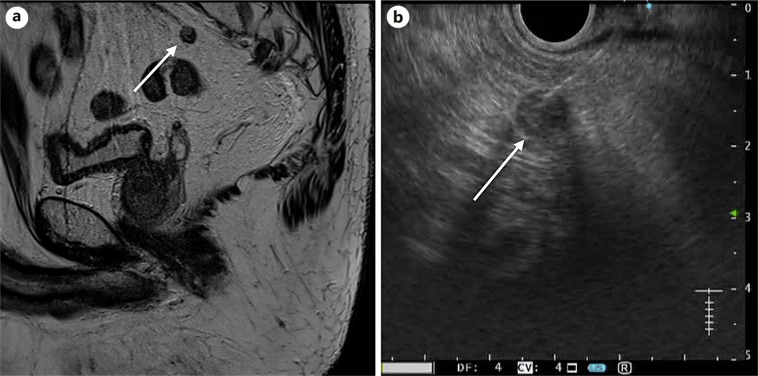
Case presentations: We report 8 cases of suspected locoregional tumor growth (LRTG) on MRI: adjacent or in the rectal wall, within the mesorectal fascia, high presacral region, and obturator foramen. MRI images were studied thoroughly before and during EUS to identify the target lesion using rectal EUS-FNA. Patients were prepared using an enema. The procedure was performed on an outpatient basis without conscious sedation. FNA was performed using a 25G needle. The patient received a 3-day course of ciprofloxacin after the procedure to prevent infection of the perirectal space. Identification of the target was the most difficult part of EUS but was successful in all cases. FNA revealed adenocarcinoma in 7 cases. Five cases were confirmed by TME results: 1 patient died before the operation, and 1 patient was treated with CRT. One patient with a suspected node in the obturator foramen was free of tumors on FNA. The TME resection specimen contained 31 lymph nodes without metastasis. All procedures were well tolerated, and no complications were observed.
Conclusion: Suspected LRTG on MRI can be confirmed using EUS-FNA. In the era of organ-preserving treatment for rectal cancer, EUS-FNA may play a supportive role when considering TME or CRT.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


