Mustafa Abdo, Henrik Watz, Frederik Trinkmann, Sabine Bohnet, Miriam Annabelle Marcella Guess, Johannes Roeben, Katharina May, Martin Reck, Benjamin-Alexander Bollmann, Susanne Stiebeler, Sabine Dettmer, Benjamin Waschki, Klaus F Rabe, Klaas Frederik Franzen, Jens Vogel-Claussen
{"title":"Oscillometry-defined Small Airway Dysfunction in Tobacco-exposed Adults with Impaired or Preserved Airflow.","authors":"Mustafa Abdo, Henrik Watz, Frederik Trinkmann, Sabine Bohnet, Miriam Annabelle Marcella Guess, Johannes Roeben, Katharina May, Martin Reck, Benjamin-Alexander Bollmann, Susanne Stiebeler, Sabine Dettmer, Benjamin Waschki, Klaus F Rabe, Klaas Frederik Franzen, Jens Vogel-Claussen","doi":"10.1164/rccm.202501-0028OC","DOIUrl":null,"url":null,"abstract":"<p><p><b>Rationale:</b> Small airway dysfunction (SAD) is a key feature of chronic obstructive pulmonary disease and might present in tobacco-exposed adults with normal spirometry. So far, the role of oscillometry-defined SAD in this population is largely unexplored. <b>Objective:</b> To investigate the prevalence of oscillometry-defined SAD and its associations with airway structural changes, quality of life (QoL), metabolic disease, and cardiovascular disease (CVD) in tobacco-exposed adults with impaired airflow or preserved airflow (PA). <b>Methods:</b> In a subcohort (<i>n</i> = 1,628) nested within a lung cancer screening trial, we assessed airway disease using pre-bronchodilator spirometry, oscillometry, and artificial intelligence-powered computed tomography. Impaired airflow included airflow obstruction (AFO) and preserved ratio impaired spirometry (PRISm). Subjects with PA, defined as FEV<sub>1</sub> and FEV<sub>1</sub>:FVC greater than the lower limit of normal, were further stratified as PA with SAD (PA-SAD) or normal lung function. SAD was defined as the frequency dependence of resistance or reactance area greater than the upper limit of normal. Computed tomography biomarkers included airway wall thickness, luminal diameter, branch count, and emphysema. QoL was measured using the euroqol 5-dimension 5-level (EQ-5D-5L). <b>Measurements and Main Results:</b> The overall prevalence of SAD was 39%. SAD was present in 26% of subjects with PA and in 60% of those with impaired airflow. The frequency of AFO, PRISm, and PA-SAD was 21%, 15%, and 16%, respectively. Similar to those with impaired airflow, subjects with PA-SAD had lower EQ-5D-5L scores, greater airway wall thickness, narrower lumen, lower branch count, and higher rate of metabolic disease and CVD than those with normal lung function (<i>P</i> < 0.01 for all). However, they had minimal emphysema and significantly higher branch count than those with AFO. Subjects with AFO or PRISm and concurrent SAD had greater structural changes and more frequent CVD than those with AFO or PRISm alone. SAD was associated with CVD (odds ratio, 1.91 [95% confidence interval, 1.55-2.36]), even after adjusting for confounders and metabolic disease. <b>Conclusions:</b> SAD is highly prevalent among tobacco-exposed adults and is associated with airway structural changes, impaired QoL, and an increased rate of CVD, even among those with PA. PA-SAD is distinct from AFO by its preserved airway count and minimal emphysema.</p>","PeriodicalId":7664,"journal":{"name":"American journal of respiratory and critical care medicine","volume":" ","pages":"1652-1661"},"PeriodicalIF":19.4000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12432392/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"American journal of respiratory and critical care medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1164/rccm.202501-0028OC","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
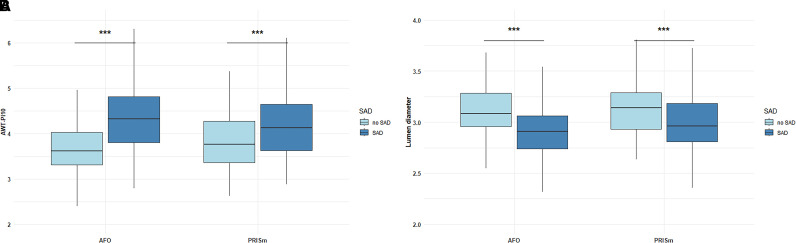
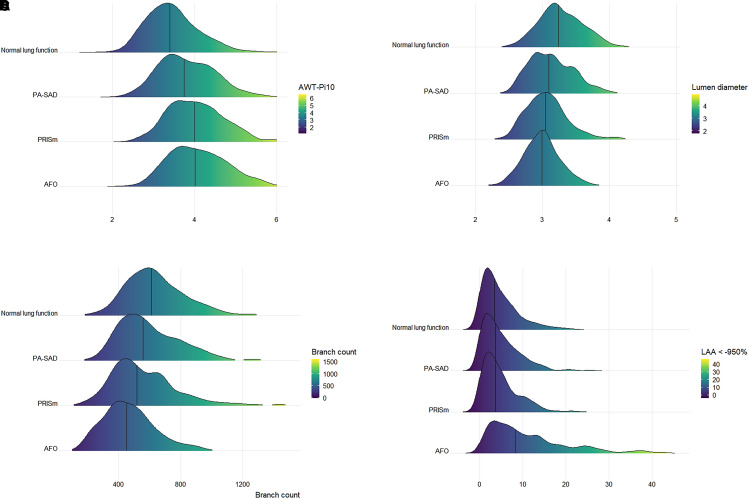
Rationale: Small airway dysfunction (SAD) is a key feature of chronic obstructive pulmonary disease and might present in tobacco-exposed adults with normal spirometry. So far, the role of oscillometry-defined SAD in this population is largely unexplored. Objective: To investigate the prevalence of oscillometry-defined SAD and its associations with airway structural changes, quality of life (QoL), metabolic disease, and cardiovascular disease (CVD) in tobacco-exposed adults with impaired airflow or preserved airflow (PA). Methods: In a subcohort (n = 1,628) nested within a lung cancer screening trial, we assessed airway disease using pre-bronchodilator spirometry, oscillometry, and artificial intelligence-powered computed tomography. Impaired airflow included airflow obstruction (AFO) and preserved ratio impaired spirometry (PRISm). Subjects with PA, defined as FEV1 and FEV1:FVC greater than the lower limit of normal, were further stratified as PA with SAD (PA-SAD) or normal lung function. SAD was defined as the frequency dependence of resistance or reactance area greater than the upper limit of normal. Computed tomography biomarkers included airway wall thickness, luminal diameter, branch count, and emphysema. QoL was measured using the euroqol 5-dimension 5-level (EQ-5D-5L). Measurements and Main Results: The overall prevalence of SAD was 39%. SAD was present in 26% of subjects with PA and in 60% of those with impaired airflow. The frequency of AFO, PRISm, and PA-SAD was 21%, 15%, and 16%, respectively. Similar to those with impaired airflow, subjects with PA-SAD had lower EQ-5D-5L scores, greater airway wall thickness, narrower lumen, lower branch count, and higher rate of metabolic disease and CVD than those with normal lung function (P < 0.01 for all). However, they had minimal emphysema and significantly higher branch count than those with AFO. Subjects with AFO or PRISm and concurrent SAD had greater structural changes and more frequent CVD than those with AFO or PRISm alone. SAD was associated with CVD (odds ratio, 1.91 [95% confidence interval, 1.55-2.36]), even after adjusting for confounders and metabolic disease. Conclusions: SAD is highly prevalent among tobacco-exposed adults and is associated with airway structural changes, impaired QoL, and an increased rate of CVD, even among those with PA. PA-SAD is distinct from AFO by its preserved airway count and minimal emphysema.
期刊介绍:
The American Journal of Respiratory and Critical Care Medicine focuses on human biology and disease, as well as animal studies that contribute to the understanding of pathophysiology and treatment of diseases that affect the respiratory system and critically ill patients. Papers that are solely or predominantly based in cell and molecular biology are published in the companion journal, the American Journal of Respiratory Cell and Molecular Biology. The Journal also seeks to publish clinical trials and outstanding review articles on areas of interest in several forms. The State-of-the-Art review is a treatise usually covering a broad field that brings bench research to the bedside. Shorter reviews are published as Critical Care Perspectives or Pulmonary Perspectives. These are generally focused on a more limited area and advance a concerted opinion about care for a specific process. Concise Clinical Reviews provide an evidence-based synthesis of the literature pertaining to topics of fundamental importance to the practice of pulmonary, critical care, and sleep medicine. Images providing advances or unusual contributions to the field are published as Images in Pulmonary, Critical Care, Sleep Medicine and the Sciences.
A recent trend and future direction of the Journal has been to include debates of a topical nature on issues of importance in pulmonary and critical care medicine and to the membership of the American Thoracic Society. Other recent changes have included encompassing works from the field of critical care medicine and the extension of the editorial governing of journal policy to colleagues outside of the United States of America. The focus and direction of the Journal is to establish an international forum for state-of-the-art respiratory and critical care medicine.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


