Prognostic value of pathological sensitivity for high-risk, localized prostate cancer receiving neoadjuvant hormonal therapy combined with radical prostatectomy.
Kai Shi, Shouzhen Chen, Xueli Wang, Wenfu Wang, Yaofeng Zhu, Bo Han, Yong Wang, Benkang Shi
{"title":"Prognostic value of pathological sensitivity for high-risk, localized prostate cancer receiving neoadjuvant hormonal therapy combined with radical prostatectomy.","authors":"Kai Shi, Shouzhen Chen, Xueli Wang, Wenfu Wang, Yaofeng Zhu, Bo Han, Yong Wang, Benkang Shi","doi":"10.1080/07853890.2025.2485399","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The exact factors influencing the prognosis of patients with prostate cancer (PCa) receiving neoadjuvant hormonal therapy (NHT) remain obscure. In our previous study, we proposed a new pathological response grading system for PCa using NHT. The aim of this study was to explore the potential prognostic value of this new system in high-risk and locally advanced PCa patients receiving NHT.</p><p><strong>Methods: </strong>We retrospectively analyzed 84 patients with high-risk locally advanced PCa. All patients received at least 3 months of NHT before radical prostatectomy (RP). The new pathological response system, the Qilu NHT pathological score (QNPS), has been described in our previous study. According to the QNPS, 84 patients were divided into two groups. 62 patients with good pathological reactions were grouped into the drug-sensitive (DS) group and 22 patients with poor pathological reactions were grouped into the drug-resistant (DR) group. Surgical outcomes and prognostic data were also analyzed.</p><p><strong>Results: </strong>Survival analysis of two groups showed that the overall survival (OS) and progression-free survival (PFS) of the DS group were both significantly longer than those of the DR group (<i>p</i> < 0.05). We further explored the prognostic values of preoperative clinical and pathological characteristics on the postoperative OS and PFS. Preoperative PSA level (<24.50 or >24.50, HR = 98.36, 95% CI 1.376-7030.033, <i>p</i> = 0.035), Gleason score (≤7 or ≥8, HR = 10.44, 95% CI 1.371-79.425, <i>p</i> = 0.024) and cribriform growth pattern were found to be associated with PFS but not OS in univariable analysis. In addition, surgical margins and ductal adenocarcinoma differentiation showed a statistically significant correlation with OS in both univariable analysis and multivariable analyses.</p><p><strong>Conclusions: </strong>The difference in pathological response of PCa patients to neoadjuvant hormonal therapy has an important influence on patient survival, and can be used as an indicator to evaluate the prognosis of PCa.</p>","PeriodicalId":93874,"journal":{"name":"Annals of medicine","volume":"57 1","pages":"2485399"},"PeriodicalIF":4.3000,"publicationDate":"2025-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11966971/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/07853890.2025.2485399","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/2 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: The exact factors influencing the prognosis of patients with prostate cancer (PCa) receiving neoadjuvant hormonal therapy (NHT) remain obscure. In our previous study, we proposed a new pathological response grading system for PCa using NHT. The aim of this study was to explore the potential prognostic value of this new system in high-risk and locally advanced PCa patients receiving NHT.
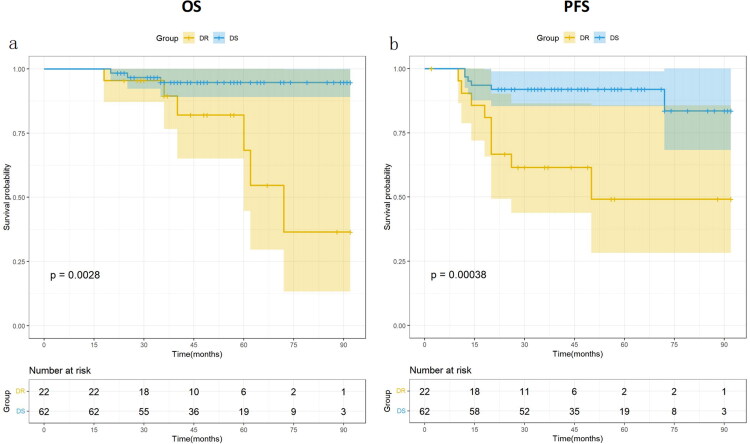
Methods: We retrospectively analyzed 84 patients with high-risk locally advanced PCa. All patients received at least 3 months of NHT before radical prostatectomy (RP). The new pathological response system, the Qilu NHT pathological score (QNPS), has been described in our previous study. According to the QNPS, 84 patients were divided into two groups. 62 patients with good pathological reactions were grouped into the drug-sensitive (DS) group and 22 patients with poor pathological reactions were grouped into the drug-resistant (DR) group. Surgical outcomes and prognostic data were also analyzed.
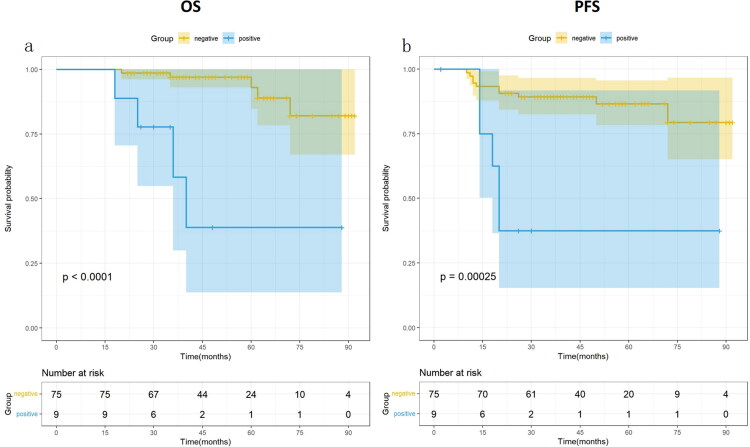
Results: Survival analysis of two groups showed that the overall survival (OS) and progression-free survival (PFS) of the DS group were both significantly longer than those of the DR group (p < 0.05). We further explored the prognostic values of preoperative clinical and pathological characteristics on the postoperative OS and PFS. Preoperative PSA level (<24.50 or >24.50, HR = 98.36, 95% CI 1.376-7030.033, p = 0.035), Gleason score (≤7 or ≥8, HR = 10.44, 95% CI 1.371-79.425, p = 0.024) and cribriform growth pattern were found to be associated with PFS but not OS in univariable analysis. In addition, surgical margins and ductal adenocarcinoma differentiation showed a statistically significant correlation with OS in both univariable analysis and multivariable analyses.
Conclusions: The difference in pathological response of PCa patients to neoadjuvant hormonal therapy has an important influence on patient survival, and can be used as an indicator to evaluate the prognosis of PCa.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


