Jiahui Zhang, Lili Xu, Gumuyang Zhang, Daming Zhang, Xiaoxiao Zhang, Xin Bai, Li Chen, Qianyu Peng, Zhengyu Jin, Hao Sun
{"title":"Multiparametric MRI to Predict Gleason Score Upgrading and Downgrading at Radical Prostatectomy Compared to Presurgical Biopsy.","authors":"Jiahui Zhang, Lili Xu, Gumuyang Zhang, Daming Zhang, Xiaoxiao Zhang, Xin Bai, Li Chen, Qianyu Peng, Zhengyu Jin, Hao Sun","doi":"10.3348/kjr.2024.1008","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study investigated the value of multiparametric MRI (mpMRI) in predicting Gleason score (GS) upgrading and downgrading in radical prostatectomy (RP) compared with presurgical biopsy.</p><p><strong>Materials and methods: </strong>Clinical and mpMRI data were retrospectively collected from 219 patients with prostate disease between January 2015 and December 2021. All patients underwent systematic prostate biopsy followed by RP. MpMRI included conventional diffusion-weighted and dynamic contrast-enhanced imaging. Multivariable logistic regression analysis was performed to analyze the factors associated with GS upgrading and downgrading after RP. Receiver operating characteristic curve analysis was used to estimate the area under the curve (AUC) to indicate the performance of the multivariable logistic regression models in predicting GS upgrade and downgrade after RP.</p><p><strong>Results: </strong>The GS after RP was upgraded, downgraded, and unchanged in 92, 43, and 84 patients, respectively. The AUCs of the clinical (percentage of positive biopsy cores [PBCs], time from biopsy to RP) and mpMRI models (prostate cancer [PCa] location, Prostate Imaging Reporting and Data System [PI-RADS] v2.1 score) for predicting GS upgrading after RP were 0.714 and 0.749, respectively. The AUC of the combined diagnostic model (age, percentage of PBCs, tPSA, PCa location, and PI-RADS v2.1 score) was 0.816, which was larger than that of the clinical factors alone (<i>P</i> < 0.001). The AUCs of the clinical (age, percentage of PBCs, ratio of free/total PSA [F/T]) and mpMRI models (PCa diameter, PCa location, and PI-RADS v2.1 score) for predicting GS downgrading after RP were 0.749 and 0.835, respectively. The AUC of the combined diagnostic model (age, percentage of PBCs, F/T, PCa diameter, PCa location, and PI-RADS v2.1 score) was 0.883, which was larger than that of the clinical factors alone (<i>P</i> < 0.001).</p><p><strong>Conclusion: </strong>Combining clinical factors and mpMRI findings can predict GS upgrade and downgrade after RP more accurately than using clinical factors alone.</p>","PeriodicalId":17881,"journal":{"name":"Korean Journal of Radiology","volume":" ","pages":"422-434"},"PeriodicalIF":5.3000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12055267/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Radiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3348/kjr.2024.1008","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/21 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: This study investigated the value of multiparametric MRI (mpMRI) in predicting Gleason score (GS) upgrading and downgrading in radical prostatectomy (RP) compared with presurgical biopsy.
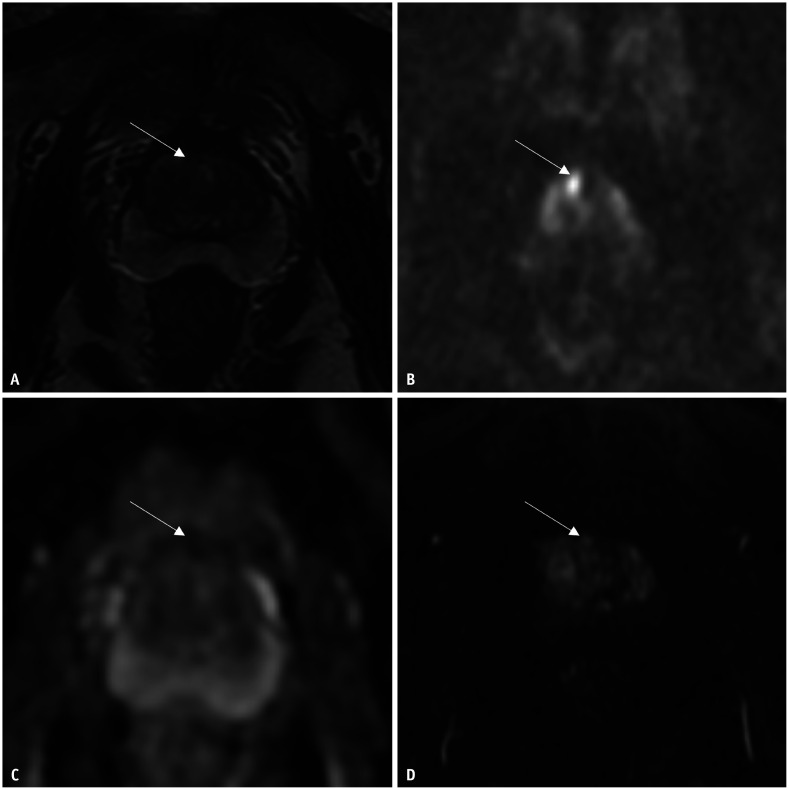
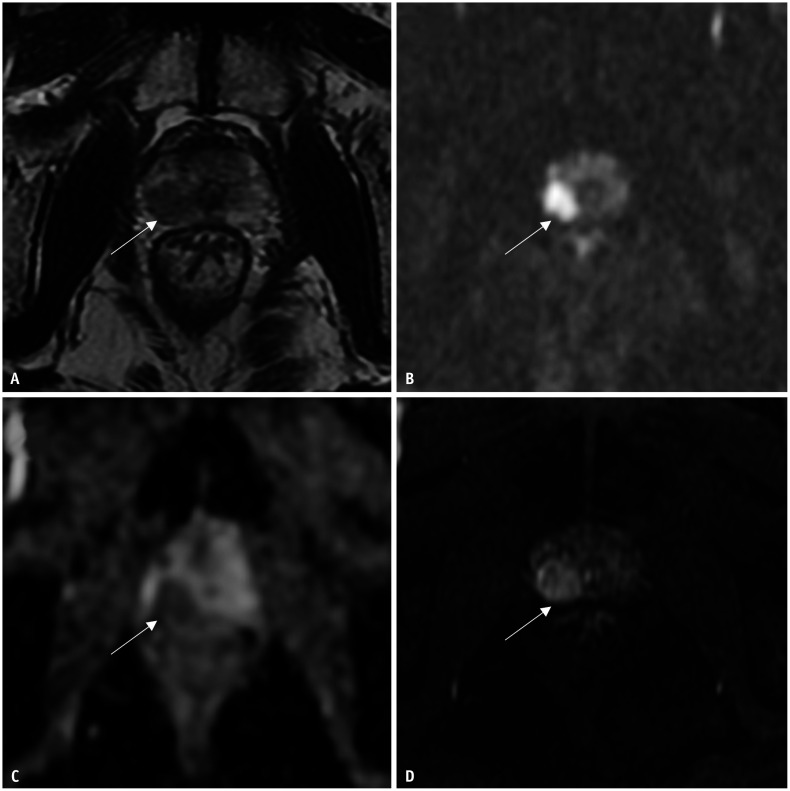
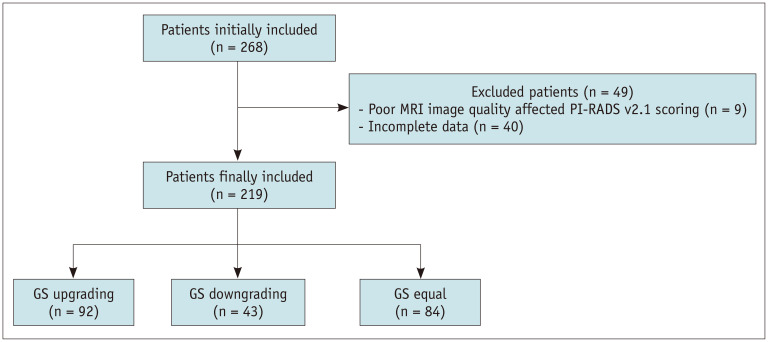
Materials and methods: Clinical and mpMRI data were retrospectively collected from 219 patients with prostate disease between January 2015 and December 2021. All patients underwent systematic prostate biopsy followed by RP. MpMRI included conventional diffusion-weighted and dynamic contrast-enhanced imaging. Multivariable logistic regression analysis was performed to analyze the factors associated with GS upgrading and downgrading after RP. Receiver operating characteristic curve analysis was used to estimate the area under the curve (AUC) to indicate the performance of the multivariable logistic regression models in predicting GS upgrade and downgrade after RP.
Results: The GS after RP was upgraded, downgraded, and unchanged in 92, 43, and 84 patients, respectively. The AUCs of the clinical (percentage of positive biopsy cores [PBCs], time from biopsy to RP) and mpMRI models (prostate cancer [PCa] location, Prostate Imaging Reporting and Data System [PI-RADS] v2.1 score) for predicting GS upgrading after RP were 0.714 and 0.749, respectively. The AUC of the combined diagnostic model (age, percentage of PBCs, tPSA, PCa location, and PI-RADS v2.1 score) was 0.816, which was larger than that of the clinical factors alone (P < 0.001). The AUCs of the clinical (age, percentage of PBCs, ratio of free/total PSA [F/T]) and mpMRI models (PCa diameter, PCa location, and PI-RADS v2.1 score) for predicting GS downgrading after RP were 0.749 and 0.835, respectively. The AUC of the combined diagnostic model (age, percentage of PBCs, F/T, PCa diameter, PCa location, and PI-RADS v2.1 score) was 0.883, which was larger than that of the clinical factors alone (P < 0.001).
Conclusion: Combining clinical factors and mpMRI findings can predict GS upgrade and downgrade after RP more accurately than using clinical factors alone.
期刊介绍:
The inaugural issue of the Korean J Radiol came out in March 2000. Our journal aims to produce and propagate knowledge on radiologic imaging and related sciences.
A unique feature of the articles published in the Journal will be their reflection of global trends in radiology combined with an East-Asian perspective. Geographic differences in disease prevalence will be reflected in the contents of papers, and this will serve to enrich our body of knowledge.
World''s outstanding radiologists from many countries are serving as editorial board of our journal.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


