Naveena Luke, Inna Carmela De Leon, Shayan Azizi, Seymour Katz
{"title":"A Case Report: Cryptogenic Multifocal Ulcerative Stenosing Enteritis - A Diagnostic Challenge Mimicking Crohn's Disease.","authors":"Naveena Luke, Inna Carmela De Leon, Shayan Azizi, Seymour Katz","doi":"10.1159/000544941","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Cryptogenic multifocal ulcerative stenosing enteritis (CMUSE) is a rare and underrecognized small bowel disorder that often mimics Crohn's disease, leading to delays in diagnosis and misdirected treatment. Given its relapsing nature and resistance to conventional inflammatory bowel disease (IBD) therapies, CMUSE presents significant diagnostic and therapeutic challenges.</p><p><strong>Case presentation: </strong>We present the case of a 41-year-old male with chronic anemia, fatigue, weight loss, and intermittent abdominal pain with melena, who remained undiagnosed for 9 years despite extensive evaluations. Imaging and endoscopy failed to identify a definitive cause, and management with TNF inhibitors and IL-12/IL-23 blockade provided only temporary relief. The patient required multiple surgical resections due to recurrent strictures. Pathological examination consistently revealed multifocal jejunal ulceration with stenosis but lacked granulomas, vasculitis, or systemic inflammatory markers, ultimately confirming CMUSE. Given its distinct pathology and treatment resistance, differentiating CMUSE from Crohn's disease is essential. The patient's ongoing management includes upadacitinib, a JAK1 inhibitor, which may help modulate immune pathways contributing to ulcer formation and stricture development.</p><p><strong>Conclusion: </strong>This case underscores the need for heightened clinical recognition of CMUSE, particularly in patients with unexplained small bowel strictures and ulceration unresponsive to standard IBD therapies. Genetic testing may aid in distinguishing CMUSE from Crohn's disease, preventing unnecessary immunosuppressive treatments. Further research is necessary to establish effective, targeted therapies and improve outcomes for patients with this rare condition.</p>","PeriodicalId":9614,"journal":{"name":"Case Reports in Gastroenterology","volume":"19 1","pages":"238-245"},"PeriodicalIF":0.6000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11961150/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000544941","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Cryptogenic multifocal ulcerative stenosing enteritis (CMUSE) is a rare and underrecognized small bowel disorder that often mimics Crohn's disease, leading to delays in diagnosis and misdirected treatment. Given its relapsing nature and resistance to conventional inflammatory bowel disease (IBD) therapies, CMUSE presents significant diagnostic and therapeutic challenges.
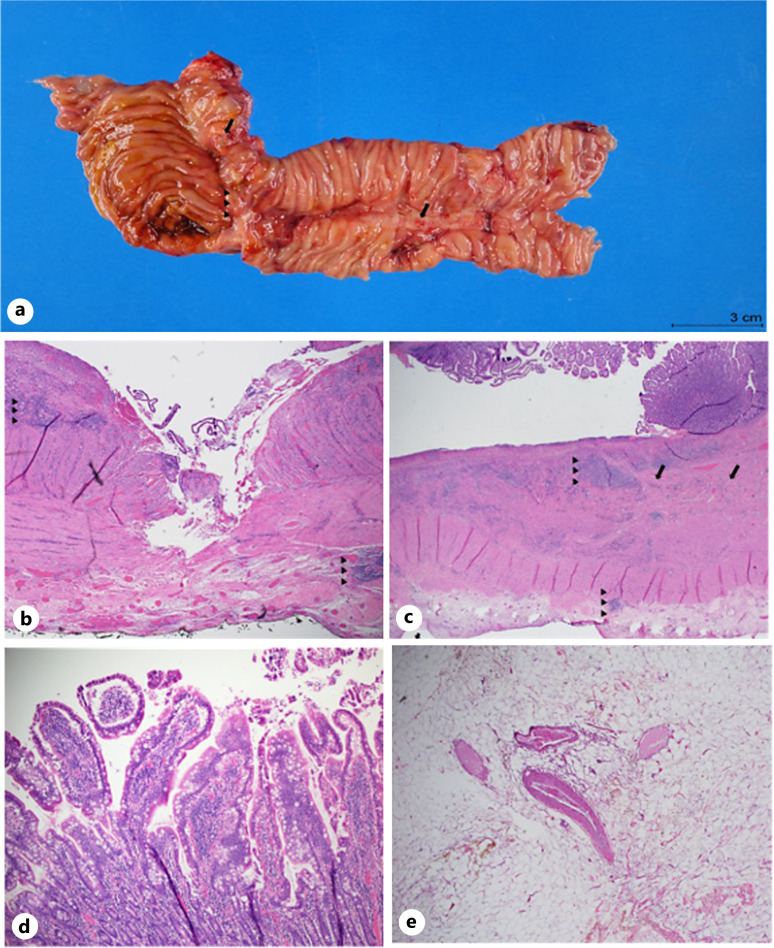
Case presentation: We present the case of a 41-year-old male with chronic anemia, fatigue, weight loss, and intermittent abdominal pain with melena, who remained undiagnosed for 9 years despite extensive evaluations. Imaging and endoscopy failed to identify a definitive cause, and management with TNF inhibitors and IL-12/IL-23 blockade provided only temporary relief. The patient required multiple surgical resections due to recurrent strictures. Pathological examination consistently revealed multifocal jejunal ulceration with stenosis but lacked granulomas, vasculitis, or systemic inflammatory markers, ultimately confirming CMUSE. Given its distinct pathology and treatment resistance, differentiating CMUSE from Crohn's disease is essential. The patient's ongoing management includes upadacitinib, a JAK1 inhibitor, which may help modulate immune pathways contributing to ulcer formation and stricture development.
Conclusion: This case underscores the need for heightened clinical recognition of CMUSE, particularly in patients with unexplained small bowel strictures and ulceration unresponsive to standard IBD therapies. Genetic testing may aid in distinguishing CMUSE from Crohn's disease, preventing unnecessary immunosuppressive treatments. Further research is necessary to establish effective, targeted therapies and improve outcomes for patients with this rare condition.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


