{"title":"Ten-year outcome of a dedicated hip fracture unit embedded within a level 1 major trauma centre.","authors":"B Ahmad, F Davis, G Chan, B A Rogers","doi":"10.1308/rcsann.2024.0094","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Fragility hip fracture (FHF) care has been revolutionised by the introduction of the best practice tariff and its associated quality assessment domains. However, increasing demands on trauma services, most notably in regional major trauma centres (MTC), have resulted in competing challenges for clinical resources. This study aims to identify whether a dedicated hip fracture unit (HFU) embedded within a trust hosting the regional MTC affords sustained improvements in clinical outcomes for FHFs.</p><p><strong>Methods: </strong>A 10-year retrospective cohort study was performed using a prospectively collected database that was cross-referenced against contemporary data submitted to the National Hip Fracture Database by a single multicentre National Health Service trust. The study period encompassed a 10-year period covering 5 years before and 5 years after formation of a dedicated HFU. The outcomes evaluated include time to surgery, length of hospital stay, discharge location and mortality.</p><p><strong>Results: </strong>Some 4,998 patients sustained FHFs: 2,387 patients (2,533 injuries) treated prior to formation of the HFU formation and 2,611 patients (2,813 injuries) treated after. The mean time to surgical intervention was significantly lower in the group treated at the HFU by 3.1 days (<i>p </i>< 0.001). Length of hospital stay was also significantly reduced at the HFU (<i>p </i>< 0.001). More patients were discharged back to their premorbid residence from the HFU (47% vs 40%). The 30- and 365-day mortality rates were significantly reduced at the HFU (<i>p </i>= 0.005 and <i>p </i>= 0.024, respectively).</p><p><strong>Conclusion: </strong>When embedded within an MTC, the HFU model is a sustainable operational structure in the medium term that provides clear clinical benefits and could be replicated nationally and internationally at similar institutions.</p>","PeriodicalId":8088,"journal":{"name":"Annals of the Royal College of Surgeons of England","volume":" ","pages":"485-489"},"PeriodicalIF":1.7000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12400454/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of the Royal College of Surgeons of England","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1308/rcsann.2024.0094","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/2 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
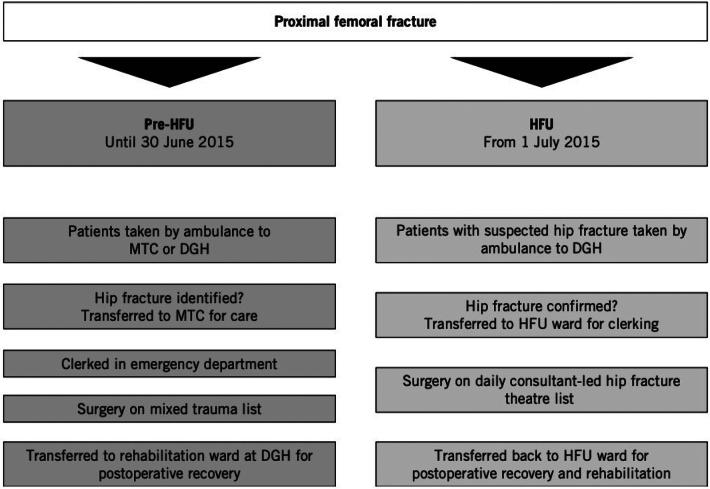
Introduction: Fragility hip fracture (FHF) care has been revolutionised by the introduction of the best practice tariff and its associated quality assessment domains. However, increasing demands on trauma services, most notably in regional major trauma centres (MTC), have resulted in competing challenges for clinical resources. This study aims to identify whether a dedicated hip fracture unit (HFU) embedded within a trust hosting the regional MTC affords sustained improvements in clinical outcomes for FHFs.
Methods: A 10-year retrospective cohort study was performed using a prospectively collected database that was cross-referenced against contemporary data submitted to the National Hip Fracture Database by a single multicentre National Health Service trust. The study period encompassed a 10-year period covering 5 years before and 5 years after formation of a dedicated HFU. The outcomes evaluated include time to surgery, length of hospital stay, discharge location and mortality.
Results: Some 4,998 patients sustained FHFs: 2,387 patients (2,533 injuries) treated prior to formation of the HFU formation and 2,611 patients (2,813 injuries) treated after. The mean time to surgical intervention was significantly lower in the group treated at the HFU by 3.1 days (p < 0.001). Length of hospital stay was also significantly reduced at the HFU (p < 0.001). More patients were discharged back to their premorbid residence from the HFU (47% vs 40%). The 30- and 365-day mortality rates were significantly reduced at the HFU (p = 0.005 and p = 0.024, respectively).
Conclusion: When embedded within an MTC, the HFU model is a sustainable operational structure in the medium term that provides clear clinical benefits and could be replicated nationally and internationally at similar institutions.
期刊介绍:
The Annals of The Royal College of Surgeons of England is the official scholarly research journal of the Royal College of Surgeons and is published eight times a year in January, February, March, April, May, July, September and November.
The main aim of the journal is to publish high-quality, peer-reviewed papers that relate to all branches of surgery. The Annals also includes letters and comments, a regular technical section, controversial topics, CORESS feedback and book reviews. The editorial board is composed of experts from all the surgical specialties.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


