Aman Goyal, Aqsa Shoaib, Areeba Fareed, Sara Jawed, Muhammad Taha Khan, Najwa Salim, Ushna Zameer, Amna Siddiqui, Tanya Thakur, Samia Aziz Sulaiman
{"title":"Outcomes of periprocedural continuation <i>vs</i> interruption of oral anticoagulation in transcatheter aortic valve replacement.","authors":"Aman Goyal, Aqsa Shoaib, Areeba Fareed, Sara Jawed, Muhammad Taha Khan, Najwa Salim, Ushna Zameer, Amna Siddiqui, Tanya Thakur, Samia Aziz Sulaiman","doi":"10.4330/wjc.v17.i3.104000","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Up to one-third of patients undergoing transcatheter aortic valve replacement (TAVR) have an indication for oral anticoagulation (OAC), primarily due to underlying atrial fibrillation. The optimal approach concerning periprocedural continuation <i>vs</i> interruption of OAC in patients undergoing TAVR remains uncertain, which our meta-analysis aims to address.</p><p><strong>Aim: </strong>To explore safety and efficacy outcomes for patients undergoing TAVR, comparing periprocedural continuation <i>vs</i> interruption of OAC therapy.</p><p><strong>Methods: </strong>A literature search was conducted across major databases to retrieve eligible studies that assessed the safety and effectiveness of TAVR with periprocedural continuous <i>vs</i> interrupted OAC. Data were pooled using a random-effects model with risk ratio (RR) and their 95% confidence interval (CI) as effect measures. All statistical analyses were conducted using Review Manager with statistical significance set at <i>P</i> < 0.05.</p><p><strong>Results: </strong>Four studies were included, encompassing a total of 1813 patients with a mean age of 80.6 years and 49.8% males. A total of 733 patients underwent OAC interruption and 1080 continued. Stroke incidence was significantly lower in the OAC continuation group (RR = 0.62, 95%CI: 0.40-0.94; <i>P</i> = 0.03). No significant differences in major vascular complications were found between the two groups (RR = 0.95, 95%CI: 0.77-1.16; <i>P</i> = 0.60) and major bleeding (RR = 0.90, 95%CI: 0.72-1.12; <i>P</i> = 0.33). All-cause mortality was non-significant between the two groups (RR = 0.83, 95%CI: 0.57-1.20; <i>P</i> = 0.32).</p><p><strong>Conclusion: </strong>Continuation of OAC significantly reduced stroke risk, whereas it showed trends toward lower bleeding and mortality that were not statistically significant. Further large-scale studies are crucial to determine clinical significance.</p>","PeriodicalId":23800,"journal":{"name":"World Journal of Cardiology","volume":"17 3","pages":"104000"},"PeriodicalIF":2.8000,"publicationDate":"2025-03-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11947949/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4330/wjc.v17.i3.104000","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Up to one-third of patients undergoing transcatheter aortic valve replacement (TAVR) have an indication for oral anticoagulation (OAC), primarily due to underlying atrial fibrillation. The optimal approach concerning periprocedural continuation vs interruption of OAC in patients undergoing TAVR remains uncertain, which our meta-analysis aims to address.
Aim: To explore safety and efficacy outcomes for patients undergoing TAVR, comparing periprocedural continuation vs interruption of OAC therapy.
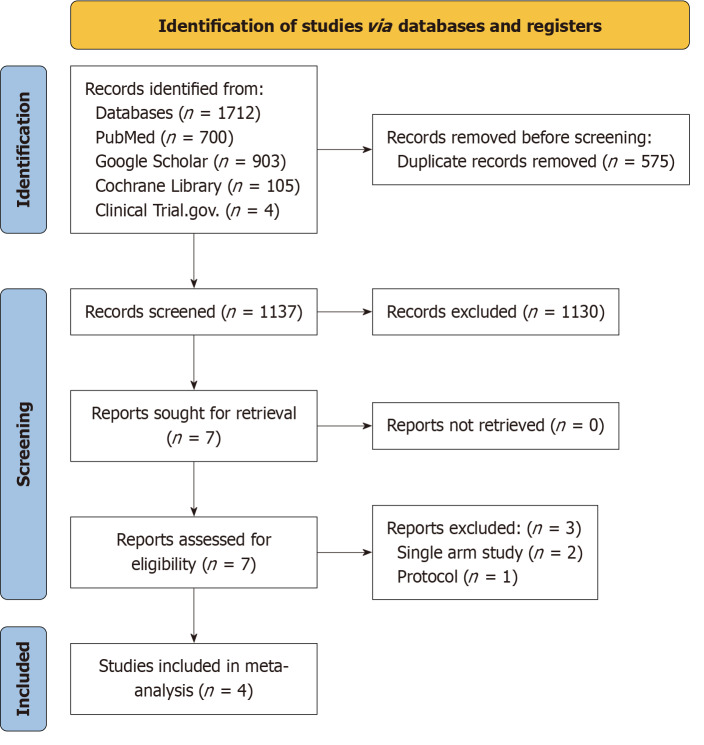
Methods: A literature search was conducted across major databases to retrieve eligible studies that assessed the safety and effectiveness of TAVR with periprocedural continuous vs interrupted OAC. Data were pooled using a random-effects model with risk ratio (RR) and their 95% confidence interval (CI) as effect measures. All statistical analyses were conducted using Review Manager with statistical significance set at P < 0.05.
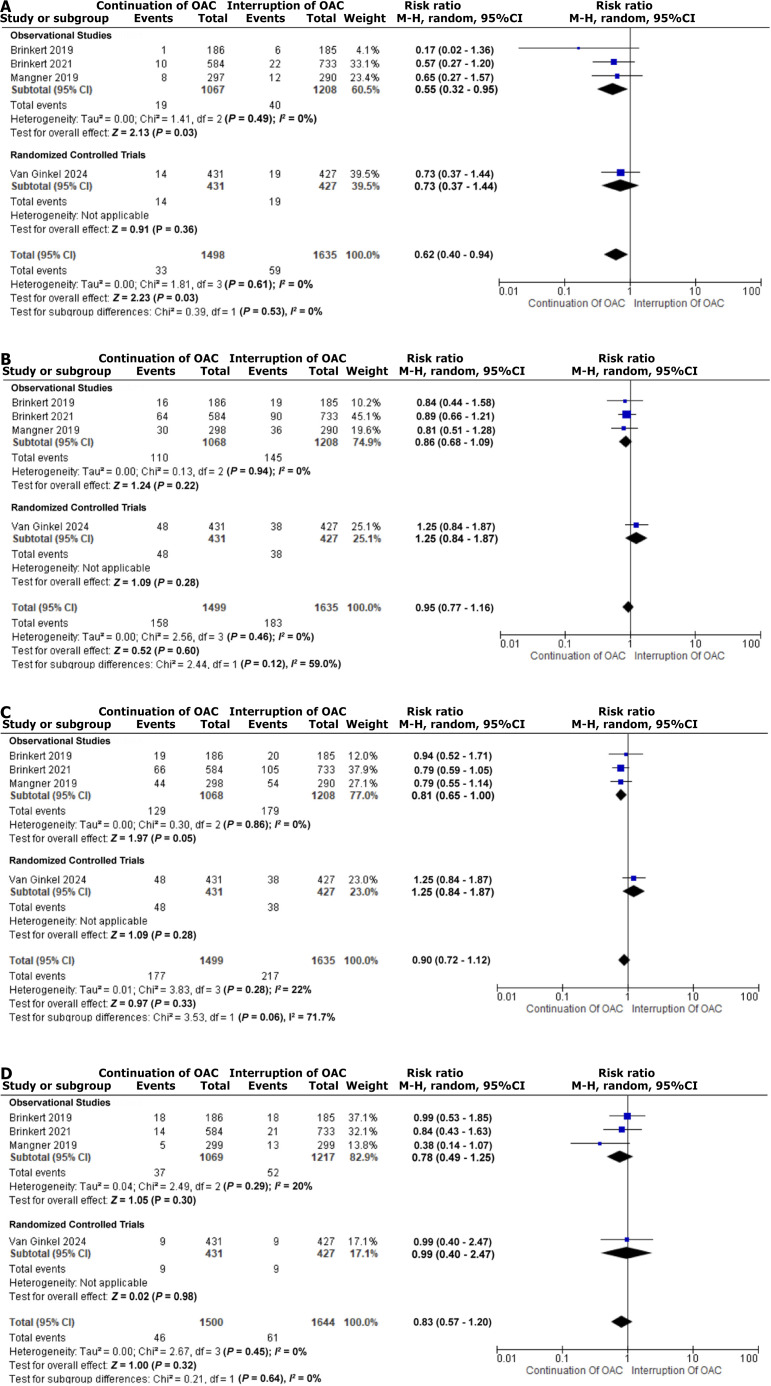
Results: Four studies were included, encompassing a total of 1813 patients with a mean age of 80.6 years and 49.8% males. A total of 733 patients underwent OAC interruption and 1080 continued. Stroke incidence was significantly lower in the OAC continuation group (RR = 0.62, 95%CI: 0.40-0.94; P = 0.03). No significant differences in major vascular complications were found between the two groups (RR = 0.95, 95%CI: 0.77-1.16; P = 0.60) and major bleeding (RR = 0.90, 95%CI: 0.72-1.12; P = 0.33). All-cause mortality was non-significant between the two groups (RR = 0.83, 95%CI: 0.57-1.20; P = 0.32).
Conclusion: Continuation of OAC significantly reduced stroke risk, whereas it showed trends toward lower bleeding and mortality that were not statistically significant. Further large-scale studies are crucial to determine clinical significance.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


