Paul Eze, Chioma Lynda Aniebo, Stanley Ilechukwu, Lucky Osaheni Lawani
{"title":"Understanding Unmet Healthcare Needs in Nigeria: Implications for Universal Health Coverage.","authors":"Paul Eze, Chioma Lynda Aniebo, Stanley Ilechukwu, Lucky Osaheni Lawani","doi":"10.1177/11786329251330032","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Many individuals in low- and middle-income countries with healthcare needs do not access the necessary, often lifesaving healthcare services. Existing universal health coverage (UHC) indicators do not account for a portion of the population with unmet healthcare needs.</p><p><strong>Objective: </strong>To estimate the prevalence, wealth-related inequality, and determinants of unmet healthcare needs in Nigeria using data from the nationally-representative Nigeria Living Standards Survey, 2018-2019.</p><p><strong>Methods: </strong>We analyzed data from a cross-sectional sample of 116 320 Nigerians from 22 110 households selected using multi-stage probability sampling. The outcome variable was self-reported unmet healthcare needs. We conducted concentration index (CIX) analyzes to assess wealth-related inequalities and performed multilevel logistic regression analysis to identify the determinants of unmet healthcare needs at the individual, household, and community levels.</p><p><strong>Results: </strong>The prevalence of unmet healthcare needs was 5.2% (95% CI: 5.0-5.5), representing about 11 million Nigerians (95% CI: 10.5-11.5 million). The most common reasons were high costs (unaffordability) and the perception that the illness or injury was not serious. Wagstaff-normalized CIX for unmet healthcare needs was pro-poor: -0.09730 for the general population and -0.10878 for those with chronic illnesses. Significant determinants of unmet healthcare needs include age (AOR: 0.99, 95% CI: 0.99-1.00), chronic illness (AOR: 8.73, 95% CI: 7.99-9.55), single-person households (AOR: 1.55, 95% CI: 1.20-2.02), poorest quintile households (AOR: 1.45, 95% CI: 1.19-1.78), and mildly (AOR: 1.17, 95% CI: 1.01-1.36) or moderately food-insecure households (AOR: 1.30, 95% CI: 1.11-1.51).</p><p><strong>Conclusion: </strong>A significant proportion of Nigerians, particularly the very poor, chronically ill, those living alone, or food insecure, have unmet healthcare needs. This highlights the necessity for targeted interventions to ensure vulnerable populations can access essential healthcare services. To progress toward UHC, the Nigerian health system must address critical issues related to healthcare accessibility.</p>","PeriodicalId":12876,"journal":{"name":"Health Services Insights","volume":"18 ","pages":"11786329251330032"},"PeriodicalIF":2.5000,"publicationDate":"2025-03-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11956516/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Services Insights","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11786329251330032","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Many individuals in low- and middle-income countries with healthcare needs do not access the necessary, often lifesaving healthcare services. Existing universal health coverage (UHC) indicators do not account for a portion of the population with unmet healthcare needs.
Objective: To estimate the prevalence, wealth-related inequality, and determinants of unmet healthcare needs in Nigeria using data from the nationally-representative Nigeria Living Standards Survey, 2018-2019.
Methods: We analyzed data from a cross-sectional sample of 116 320 Nigerians from 22 110 households selected using multi-stage probability sampling. The outcome variable was self-reported unmet healthcare needs. We conducted concentration index (CIX) analyzes to assess wealth-related inequalities and performed multilevel logistic regression analysis to identify the determinants of unmet healthcare needs at the individual, household, and community levels.
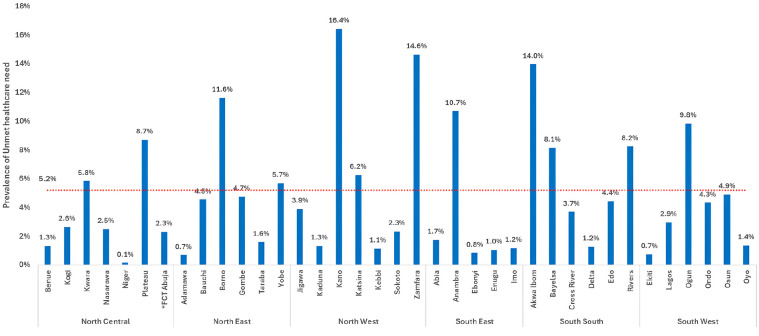
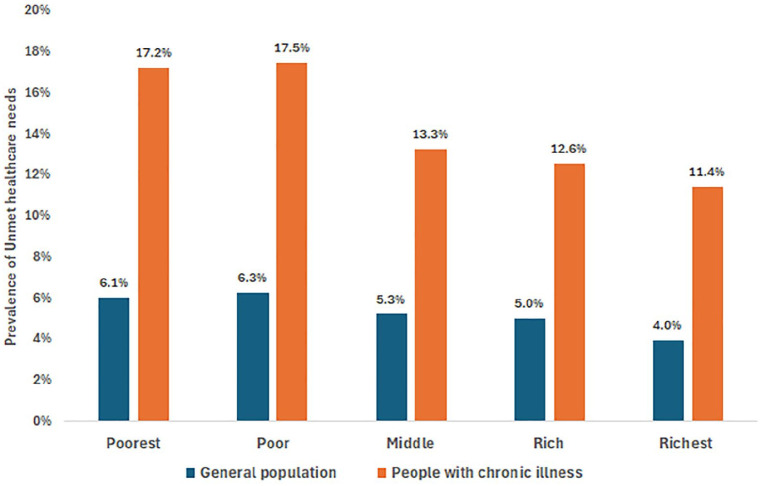
Results: The prevalence of unmet healthcare needs was 5.2% (95% CI: 5.0-5.5), representing about 11 million Nigerians (95% CI: 10.5-11.5 million). The most common reasons were high costs (unaffordability) and the perception that the illness or injury was not serious. Wagstaff-normalized CIX for unmet healthcare needs was pro-poor: -0.09730 for the general population and -0.10878 for those with chronic illnesses. Significant determinants of unmet healthcare needs include age (AOR: 0.99, 95% CI: 0.99-1.00), chronic illness (AOR: 8.73, 95% CI: 7.99-9.55), single-person households (AOR: 1.55, 95% CI: 1.20-2.02), poorest quintile households (AOR: 1.45, 95% CI: 1.19-1.78), and mildly (AOR: 1.17, 95% CI: 1.01-1.36) or moderately food-insecure households (AOR: 1.30, 95% CI: 1.11-1.51).
Conclusion: A significant proportion of Nigerians, particularly the very poor, chronically ill, those living alone, or food insecure, have unmet healthcare needs. This highlights the necessity for targeted interventions to ensure vulnerable populations can access essential healthcare services. To progress toward UHC, the Nigerian health system must address critical issues related to healthcare accessibility.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


