Gudrun M Feuchtner, Pietro G Lacaita, Jeroen J Bax, Fatima Rodriguez, Rine Nakanishi, Gianluca Pontone, Saima Mushtaq, Ronny R Buechel, Christoph Gräni, Amit R Patel, Cristiane C Singulane, Andrew D Choi, Mouaz Al-Mallah, Daniele Andreini, Ronald P Karlsberg, Geoffrey Cho, Carlos E Rochitte, Mirvat Alasnag, Ashraf Hamdan, Filippo Cademartiri, Erica Maffei, Hugo Marques, Pedro M Gonçalves Pereira, Himanshu Gupta, Martin Hadamitzky, Omar Khalique, Dinesh Kalra, James D Mills, Nick S Nurmohamed, Paul Knaapen, Matthew Budoff, Kashif Shaikh, Enrico Martin, David M German, Maros Ferencik, Andrew C Oehler, Roderick Deaño, Prashant Nagpal, Marly Van Assen, Carlo Nicola De Cecco, Borek Foldyna, Jan Michael Brendel, Victor Y Cheng, Kelley Branch, Marcio Bittencourt, Sabha Bhatti, Venkateshwar Polsani, George Wesbey, Rhanderson Cardoso, Ron Blankstein, Augustin Delago, Amit Pursnani, Amro Alsaid, Stephen Bloom, Vasileios Kamperidis, Fabian Barbieri, Melissa Aquino, Ibrahim Danad, Alexander van Rosendael
{"title":"AI-Quantitative CT Coronary Plaque Features Associate With a Higher Relative Risk in Women: CONFIRM2 Registry.","authors":"Gudrun M Feuchtner, Pietro G Lacaita, Jeroen J Bax, Fatima Rodriguez, Rine Nakanishi, Gianluca Pontone, Saima Mushtaq, Ronny R Buechel, Christoph Gräni, Amit R Patel, Cristiane C Singulane, Andrew D Choi, Mouaz Al-Mallah, Daniele Andreini, Ronald P Karlsberg, Geoffrey Cho, Carlos E Rochitte, Mirvat Alasnag, Ashraf Hamdan, Filippo Cademartiri, Erica Maffei, Hugo Marques, Pedro M Gonçalves Pereira, Himanshu Gupta, Martin Hadamitzky, Omar Khalique, Dinesh Kalra, James D Mills, Nick S Nurmohamed, Paul Knaapen, Matthew Budoff, Kashif Shaikh, Enrico Martin, David M German, Maros Ferencik, Andrew C Oehler, Roderick Deaño, Prashant Nagpal, Marly Van Assen, Carlo Nicola De Cecco, Borek Foldyna, Jan Michael Brendel, Victor Y Cheng, Kelley Branch, Marcio Bittencourt, Sabha Bhatti, Venkateshwar Polsani, George Wesbey, Rhanderson Cardoso, Ron Blankstein, Augustin Delago, Amit Pursnani, Amro Alsaid, Stephen Bloom, Vasileios Kamperidis, Fabian Barbieri, Melissa Aquino, Ibrahim Danad, Alexander van Rosendael","doi":"10.1161/CIRCIMAGING.125.018235","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Coronary plaque features are imaging biomarkers of cardiovascular risk, but less is known about sex-specific patterns in their prognostic value. This study aimed to define sex differences in the coronary atherosclerotic phenotypes assessed by artificial intelligence-based quantitative computed tomography (AI-QCT) and the associated risk of major adverse cardiovascular events (MACEs).</p><p><strong>Methods: </strong>Global multicenter registry including symptomatic patients with suspicion of coronary artery disease referred for coronary computed tomography angiography. AI-QCT analyzed 16 coronary artery disease features. The primary end point was MACE defined as death, myocardial infarction, late revascularization, cerebrovascular events, unstable angina, and congestive heart failure.</p><p><strong>Results: </strong>Among 3551 patients (mean age, 59±12 years; 49.5% women), MACE occurred in 3.2% of women and 6.1% of men during an average follow-up of 4.8±2.2 years. The AI-QCT features total plaque volume, noncalcified plaque, calcified plaque, and percentage atheroma volume were significantly higher in men (<i>P</i><0.001), and high-risk plaques were more prevalent (9.2% versus 2.5%; <i>P</i><0.0001). Independent of age and cardiovascular risk factors, the AI-QCT-derived features of total plaque volume, noncalcified plaque, calcified plaque, and percentage atheroma volume conferred a higher relative risk of MACE in women than men. For every 50-mm<sup>3</sup> increase in total plaque volume, relative risk increased by 17.7% (95% CI, 1.12-1.24) in women versus 5.3% (95% CI, 1.03-1.07) in men (<i>P</i><sub>interaction</sub><0.001); for noncalcified plaque, relative risk increased by 27.1% (95% CI, 1.17-1.38) versus 11.6% (95% CI, 1.08-1.15; <i>P</i><sub>interaction</sub>=0.0015); and for calcified plaque, relative risk increased by 22.9% (95% CI, 1.14-1.33) versus 5.4% (95% CI, 1.01-1.10; <i>P</i><sub>interaction</sub>=0.0012), respectively. Similarly, for percentage atheroma volume, the risk was higher in women. The findings remained unchanged when restricted to a secondary composite end point (death and myocardial infarction).</p><p><strong>Conclusions: </strong>The AI-QCT plaque features, total plaque volume, noncalcified plaque, calcified plaque, and percentage atheroma volume, conferred a higher relative MACE risk in women and may prompt more aggressive antiatherosclerotic therapy and reinforced preventive interventions.</p><p><strong>Registration: </strong>URL: https://www.clinicaltrials.gov; Unique identifier: NCT04279496.</p>","PeriodicalId":10202,"journal":{"name":"Circulation: Cardiovascular Imaging","volume":" ","pages":"e018235"},"PeriodicalIF":7.0000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12173162/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Circulation: Cardiovascular Imaging","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1161/CIRCIMAGING.125.018235","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/31 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Coronary plaque features are imaging biomarkers of cardiovascular risk, but less is known about sex-specific patterns in their prognostic value. This study aimed to define sex differences in the coronary atherosclerotic phenotypes assessed by artificial intelligence-based quantitative computed tomography (AI-QCT) and the associated risk of major adverse cardiovascular events (MACEs).
Methods: Global multicenter registry including symptomatic patients with suspicion of coronary artery disease referred for coronary computed tomography angiography. AI-QCT analyzed 16 coronary artery disease features. The primary end point was MACE defined as death, myocardial infarction, late revascularization, cerebrovascular events, unstable angina, and congestive heart failure.
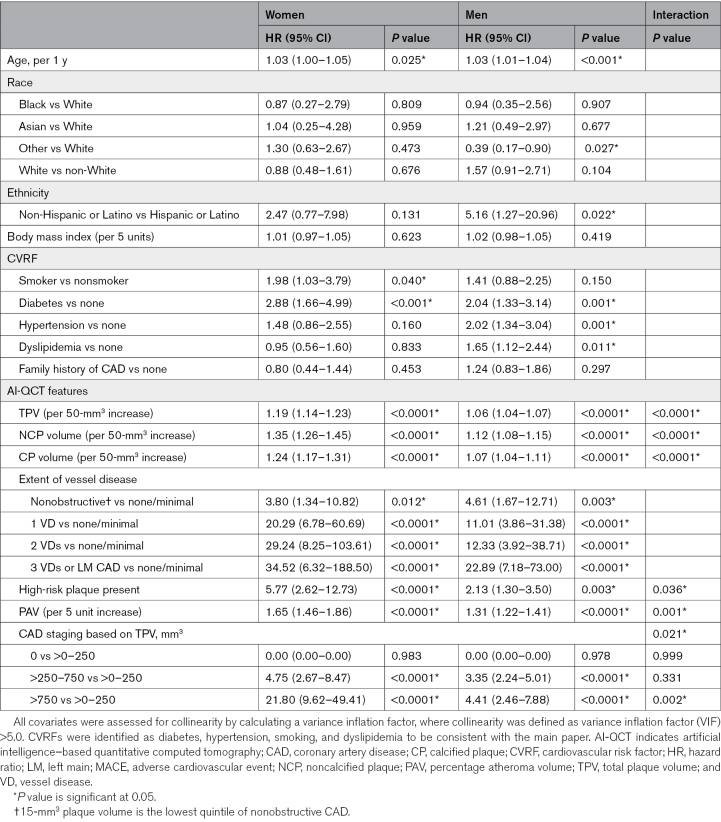
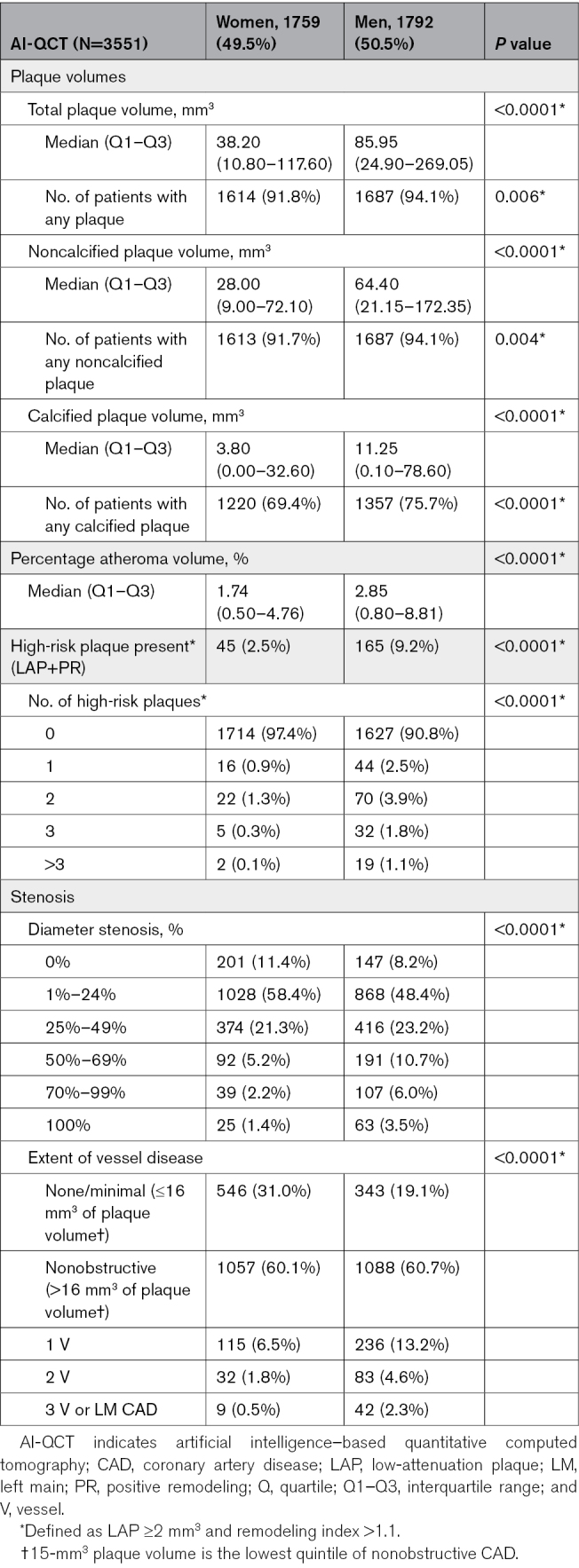
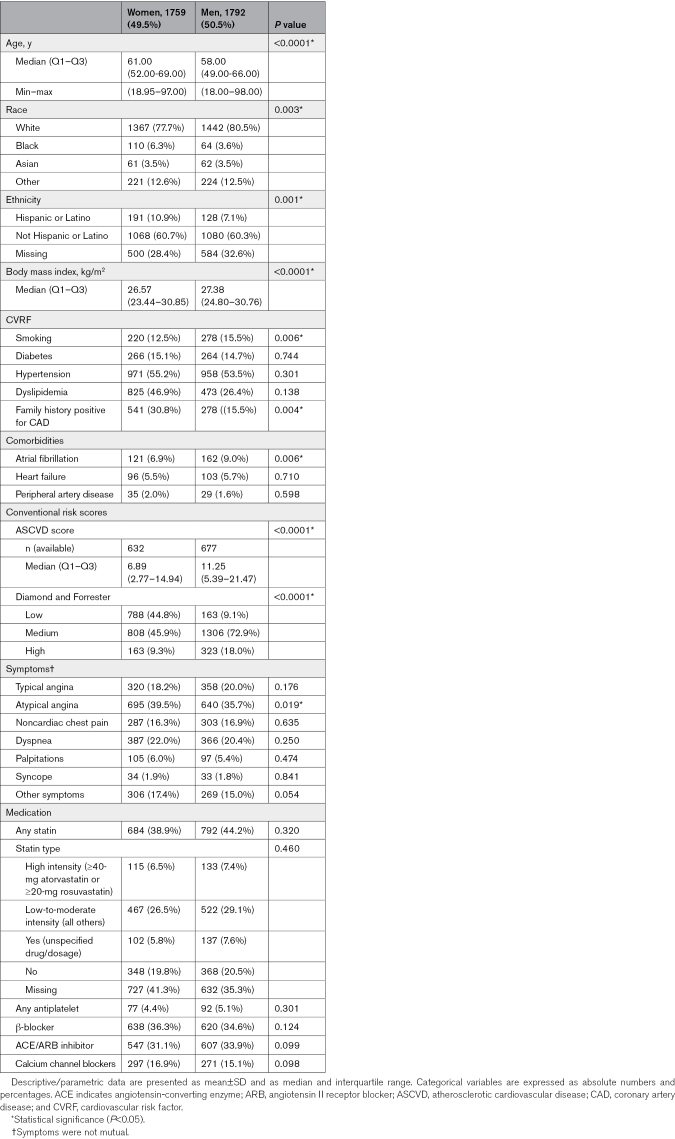
Results: Among 3551 patients (mean age, 59±12 years; 49.5% women), MACE occurred in 3.2% of women and 6.1% of men during an average follow-up of 4.8±2.2 years. The AI-QCT features total plaque volume, noncalcified plaque, calcified plaque, and percentage atheroma volume were significantly higher in men (P<0.001), and high-risk plaques were more prevalent (9.2% versus 2.5%; P<0.0001). Independent of age and cardiovascular risk factors, the AI-QCT-derived features of total plaque volume, noncalcified plaque, calcified plaque, and percentage atheroma volume conferred a higher relative risk of MACE in women than men. For every 50-mm3 increase in total plaque volume, relative risk increased by 17.7% (95% CI, 1.12-1.24) in women versus 5.3% (95% CI, 1.03-1.07) in men (Pinteraction<0.001); for noncalcified plaque, relative risk increased by 27.1% (95% CI, 1.17-1.38) versus 11.6% (95% CI, 1.08-1.15; Pinteraction=0.0015); and for calcified plaque, relative risk increased by 22.9% (95% CI, 1.14-1.33) versus 5.4% (95% CI, 1.01-1.10; Pinteraction=0.0012), respectively. Similarly, for percentage atheroma volume, the risk was higher in women. The findings remained unchanged when restricted to a secondary composite end point (death and myocardial infarction).
Conclusions: The AI-QCT plaque features, total plaque volume, noncalcified plaque, calcified plaque, and percentage atheroma volume, conferred a higher relative MACE risk in women and may prompt more aggressive antiatherosclerotic therapy and reinforced preventive interventions.
期刊介绍:
Circulation: Cardiovascular Imaging, an American Heart Association journal, publishes high-quality, patient-centric articles focusing on observational studies, clinical trials, and advances in applied (translational) research. The journal features innovative, multimodality approaches to the diagnosis and risk stratification of cardiovascular disease. Modalities covered include echocardiography, cardiac computed tomography, cardiac magnetic resonance imaging and spectroscopy, magnetic resonance angiography, cardiac positron emission tomography, noninvasive assessment of vascular and endothelial function, radionuclide imaging, molecular imaging, and others.
Article types considered by Circulation: Cardiovascular Imaging include Original Research, Research Letters, Advances in Cardiovascular Imaging, Clinical Implications of Molecular Imaging Research, How to Use Imaging, Translating Novel Imaging Technologies into Clinical Applications, and Cardiovascular Images.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


