Xiao Chen, Daniel M Blumberger, Chao-Gan Yan, Jonathan Downar, Fidel Vila-Rodriguez, Zafiris J Daskalakis, Tyler S Kaster
{"title":"Crosswalk between HRSD and MADRS outcomes for rTMS in patients with depression.","authors":"Xiao Chen, Daniel M Blumberger, Chao-Gan Yan, Jonathan Downar, Fidel Vila-Rodriguez, Zafiris J Daskalakis, Tyler S Kaster","doi":"10.1136/bmjment-2024-301451","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Hamilton Rating Scale for Depression (HRSD) and the Montgomery-Åsberg Depression Rating Scale (MADRS) are the two most common clinician-rated scales to quantify depression symptom change in repetitive transcranial magnetic stimulation (rTMS) trials. However, it is unclear how the values of one scale translate to the other. Being able to translate scores between these scales could allow for aggregating rTMS clinical trial data.</p><p><strong>Methods: </strong>Clinical data from two randomised rTMS clinical trials (FOURD and CARTBIND, total N=380) were pooled. We used five crosswalk models: (1) a pharmacotherapy equipercentile model, (2) an rTMS equipercentile model, (3) a linear regression model, (4) a random forest (RF) regression model and (5) a support vector regression (SVR) model. Model performance was benchmarked using the root mean square error (RMSE).</p><p><strong>Results: </strong>The linear regression model demonstrated the best performance (RMSE: 2.66-4.82), though the SVR model's performance was slightly worse but comparable (RMSE: 2.69-5.32). The RF regression model generally performed worst (RMSE: 2.70-5.20). The rTMS equipercentile model's performance was intermediate (RMSE: 2.69-5.32) in the primary analysis but achieved superior performance and demonstrated less bias in the additional analysis.</p><p><strong>Interpretation: </strong>MADRS and HRSD scores from rTMS trials can be accurately converted between each other. The optimal model was the newly developed equipercentile model, though the results of the SVR model were promising. Nevertheless, independent external replication is required to demonstrate the external validity of these findings.</p><p><strong>Trial registration number: </strong>FOURD: NCT02998580; CARTBIND: NCT02729792.</p>","PeriodicalId":72434,"journal":{"name":"BMJ mental health","volume":"28 1","pages":""},"PeriodicalIF":4.9000,"publicationDate":"2025-03-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11956309/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ mental health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjment-2024-301451","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"0","JCRName":"PSYCHIATRY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The Hamilton Rating Scale for Depression (HRSD) and the Montgomery-Åsberg Depression Rating Scale (MADRS) are the two most common clinician-rated scales to quantify depression symptom change in repetitive transcranial magnetic stimulation (rTMS) trials. However, it is unclear how the values of one scale translate to the other. Being able to translate scores between these scales could allow for aggregating rTMS clinical trial data.
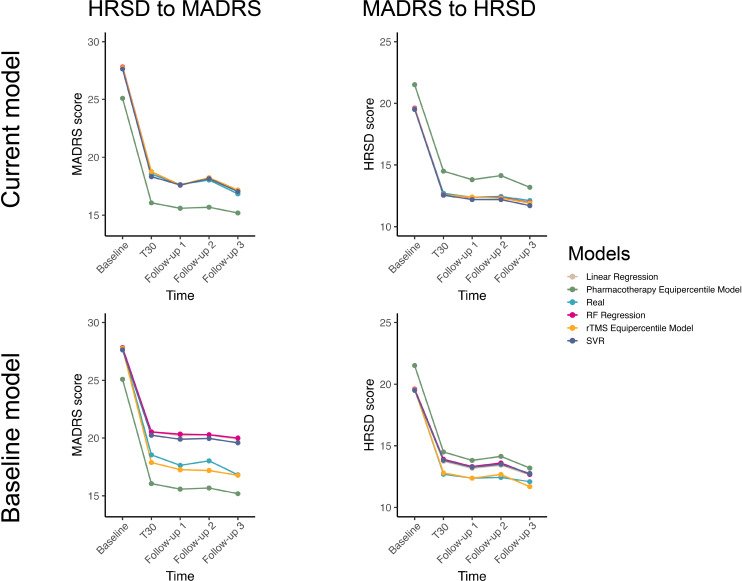
Methods: Clinical data from two randomised rTMS clinical trials (FOURD and CARTBIND, total N=380) were pooled. We used five crosswalk models: (1) a pharmacotherapy equipercentile model, (2) an rTMS equipercentile model, (3) a linear regression model, (4) a random forest (RF) regression model and (5) a support vector regression (SVR) model. Model performance was benchmarked using the root mean square error (RMSE).
Results: The linear regression model demonstrated the best performance (RMSE: 2.66-4.82), though the SVR model's performance was slightly worse but comparable (RMSE: 2.69-5.32). The RF regression model generally performed worst (RMSE: 2.70-5.20). The rTMS equipercentile model's performance was intermediate (RMSE: 2.69-5.32) in the primary analysis but achieved superior performance and demonstrated less bias in the additional analysis.
Interpretation: MADRS and HRSD scores from rTMS trials can be accurately converted between each other. The optimal model was the newly developed equipercentile model, though the results of the SVR model were promising. Nevertheless, independent external replication is required to demonstrate the external validity of these findings.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


