{"title":"Travel to low- and middle-income countries and travellers' diarrhoea increase risk of mismatching antimicrobial therapy for urinary tract infection.","authors":"Anu Patjas, Anu Kantele","doi":"10.1093/jtm/taaf025","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Travel to low- and middle-income countries (LMICs) increases the risk of urinary tract infections (UTIs), including those caused by extended-spectrum beta-lactamase-producing Enterobacterales (ESBL-PE). Focusing on international travel, we explored resistance profiles of urinary ESBL-PE and non-ESBL-PE isolates in a low antimicrobial resistance prevalence country and factors associated with UTI treatment failure.</p><p><strong>Methods: </strong>During 2015-19, we recruited 18-65-year-old individuals with recent ESBL-PE UTI and a respective cohort of those with non-ESBL-PE UTI to complete questionnaires on symptoms, antibiotic therapies and treatment failure risk factors. We compared uropathogens' resistance profiles amongst patients with or without LMIC travel history and conducted multivariable analyses to identify factors contributing to mismatching antimicrobial treatment (uropathogen resistant to the initial antimicrobial used) and clinical failure.</p><p><strong>Results: </strong>Amongst non-ESBL-PE UTI patients (n = 187), trimethoprim resistance was more common in isolates from individuals with recent LMIC travel (8/19, 42.1%) compared to those without (30/167, 18.0%) [odds ratio (OR) 3.3, compatibility interval (CI) 95% 1.2-9.0]. ESBL-PE isolates (n = 130) showed no differences in resistance profiles with respect to LMIC travel history.In the group non-ESBL-PE UTI, risk factors included microbiological mismatching recent LMIC travel [adjusted odds ratio (AOR) 3.6, CI 95% 1.0-12.7] and travellers' diarrhoea (AOR 7.1, CI 95% 1.1-45.6); no factors were significantly associated with mismatching in the group ESBL-PE UTI. As risk factors for clinical failure, in the group non-ESBL-PE UTI, we identified microbiological mismatching (AOR 15.2, CI 95% 4.0-57.9), and renal/bladder disease (AOR 5.2, CI 95% 1.1-23.2), and in the group ESBL-PE UTI, microbiological mismatching (AOR 8.1, CI 95% 2.6-24.7).</p><p><strong>Conclusions: </strong>LMIC travel increases the risk of nonmatching empiric antimicrobials, concurring with increased trimethoprim resistance rates amongst the non-ESBL-PE isolates. Our data suggest that UTI patients with recent LMIC travel should not be empirically treated with trimethoprim and, when possible, urinary culturing is warranted.</p>","PeriodicalId":17407,"journal":{"name":"Journal of travel medicine","volume":" ","pages":""},"PeriodicalIF":6.4000,"publicationDate":"2025-04-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12118056/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of travel medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/jtm/taaf025","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Travel to low- and middle-income countries (LMICs) increases the risk of urinary tract infections (UTIs), including those caused by extended-spectrum beta-lactamase-producing Enterobacterales (ESBL-PE). Focusing on international travel, we explored resistance profiles of urinary ESBL-PE and non-ESBL-PE isolates in a low antimicrobial resistance prevalence country and factors associated with UTI treatment failure.
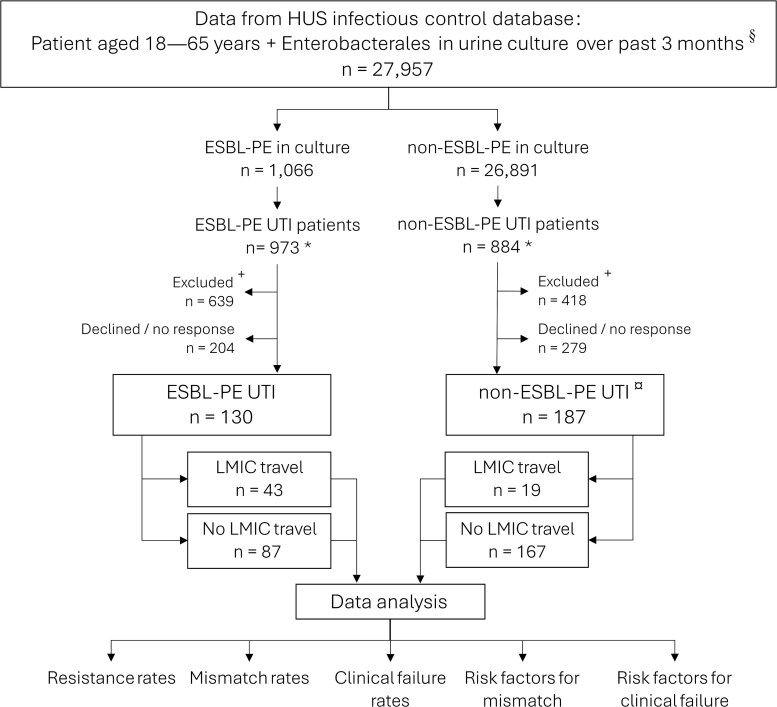
Methods: During 2015-19, we recruited 18-65-year-old individuals with recent ESBL-PE UTI and a respective cohort of those with non-ESBL-PE UTI to complete questionnaires on symptoms, antibiotic therapies and treatment failure risk factors. We compared uropathogens' resistance profiles amongst patients with or without LMIC travel history and conducted multivariable analyses to identify factors contributing to mismatching antimicrobial treatment (uropathogen resistant to the initial antimicrobial used) and clinical failure.
Results: Amongst non-ESBL-PE UTI patients (n = 187), trimethoprim resistance was more common in isolates from individuals with recent LMIC travel (8/19, 42.1%) compared to those without (30/167, 18.0%) [odds ratio (OR) 3.3, compatibility interval (CI) 95% 1.2-9.0]. ESBL-PE isolates (n = 130) showed no differences in resistance profiles with respect to LMIC travel history.In the group non-ESBL-PE UTI, risk factors included microbiological mismatching recent LMIC travel [adjusted odds ratio (AOR) 3.6, CI 95% 1.0-12.7] and travellers' diarrhoea (AOR 7.1, CI 95% 1.1-45.6); no factors were significantly associated with mismatching in the group ESBL-PE UTI. As risk factors for clinical failure, in the group non-ESBL-PE UTI, we identified microbiological mismatching (AOR 15.2, CI 95% 4.0-57.9), and renal/bladder disease (AOR 5.2, CI 95% 1.1-23.2), and in the group ESBL-PE UTI, microbiological mismatching (AOR 8.1, CI 95% 2.6-24.7).
Conclusions: LMIC travel increases the risk of nonmatching empiric antimicrobials, concurring with increased trimethoprim resistance rates amongst the non-ESBL-PE isolates. Our data suggest that UTI patients with recent LMIC travel should not be empirically treated with trimethoprim and, when possible, urinary culturing is warranted.
期刊介绍:
The Journal of Travel Medicine is a publication that focuses on travel medicine and its intersection with other disciplines. It publishes cutting-edge research, consensus papers, policy papers, and expert reviews. The journal is affiliated with the Asia Pacific Travel Health Society.
The journal's main areas of interest include the prevention and management of travel-associated infections, non-communicable diseases, vaccines, malaria prevention and treatment, multi-drug resistant pathogens, and surveillance on all individuals crossing international borders.
The Journal of Travel Medicine is indexed in multiple major indexing services, including Adis International Ltd., CABI, EBSCOhost, Elsevier BV, Gale, Journal Watch Infectious Diseases (Online), MetaPress, National Library of Medicine, OCLC, Ovid, ProQuest, Thomson Reuters, and the U.S. National Library of Medicine.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


