Laura Pini, Jordan Giordani, Guido Levi, Michele Guerini, Simone Piva, Elena Peli, Manuela Violini, Stefano Piras, Yehia El Masri, Alessandro Pini, Dina Visca, Deodato Assanelli, Maria Lorenza Muiesan, Nicola Latronico, Claudio Tantucci
{"title":"Long-term alveolar-capillary diffusion impairments after severe SARS-CoV-2 pneumonia.","authors":"Laura Pini, Jordan Giordani, Guido Levi, Michele Guerini, Simone Piva, Elena Peli, Manuela Violini, Stefano Piras, Yehia El Masri, Alessandro Pini, Dina Visca, Deodato Assanelli, Maria Lorenza Muiesan, Nicola Latronico, Claudio Tantucci","doi":"10.1080/07853890.2025.2483383","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Persistent respiratory symptoms and impaired gas exchange are common in patients recovering from COVID-19 pneumonia. The Lung Diffusing Capacity for Carbon Monoxide (DLCO) and Carbon Monoxide Transfer Coefficient (KCO) do not adequately distinguish alveolar membrane dysfunction from vascular abnormalities. This study aimed to characterize persistent diffusion impairment in post-ICU patients with prior SARS-CoV-2 pneumonia and reduced DLCO.</p><p><strong>Methods: </strong>After hospital discharge, patients underwent spirometry, DLCO measurement, and a 6-minute walking test every six months. If DLCO remained impaired at 18-24 months, a combined Lung Diffusing Capacity for Nitric Oxide (DLNO) and DLCO assessment was performed to differentiate alveolar-capillary membrane (DmCO) and pulmonary capillary blood volume (Vc) alterations.</p><p><strong>Results: </strong>Among 20 patients with persistent DLCO reduction, 3 had an obstructive ventilatory pattern, 6 had restriction, and 12 had low KCO. In restrictive cases, KCO was reduced but remained within normal limits without compensation. The DLNO/DLCO ratio exceeded 113.5% predicted in all patients. DmCO was impaired in 7 patients, while Vc was reduced in 16.</p><p><strong>Conclusion: </strong>Both DLCO determinants were affected, with vascular impairment predominating. Vc reduction was present in most patients, with mean values below the lower limit of normality, whereas DmCO was less affected and often normal. The elevated DLNO/DLCO ratio suggests that persistent DLCO reduction is primarily driven by prolonged pulmonary capillary circulation dysfunction rather than alveolar membrane alterations, highlighting the vascular component as the primary site of long-term impairment.</p>","PeriodicalId":93874,"journal":{"name":"Annals of medicine","volume":"57 1","pages":"2483383"},"PeriodicalIF":4.3000,"publicationDate":"2025-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11956098/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/07853890.2025.2483383","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/28 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Persistent respiratory symptoms and impaired gas exchange are common in patients recovering from COVID-19 pneumonia. The Lung Diffusing Capacity for Carbon Monoxide (DLCO) and Carbon Monoxide Transfer Coefficient (KCO) do not adequately distinguish alveolar membrane dysfunction from vascular abnormalities. This study aimed to characterize persistent diffusion impairment in post-ICU patients with prior SARS-CoV-2 pneumonia and reduced DLCO.
Methods: After hospital discharge, patients underwent spirometry, DLCO measurement, and a 6-minute walking test every six months. If DLCO remained impaired at 18-24 months, a combined Lung Diffusing Capacity for Nitric Oxide (DLNO) and DLCO assessment was performed to differentiate alveolar-capillary membrane (DmCO) and pulmonary capillary blood volume (Vc) alterations.
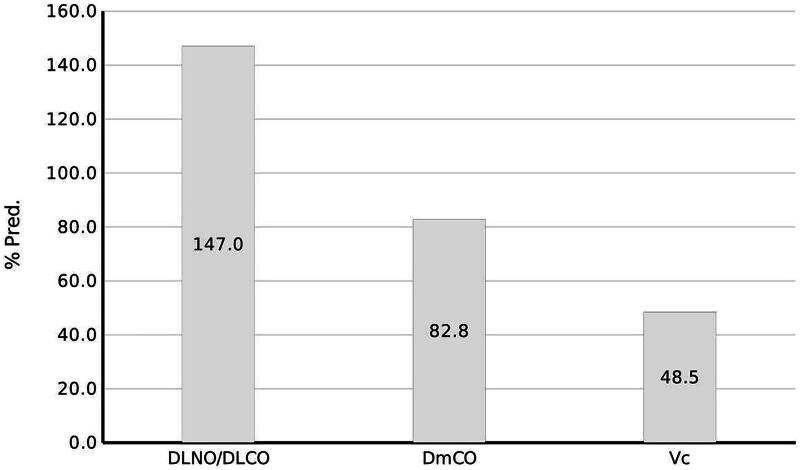
Results: Among 20 patients with persistent DLCO reduction, 3 had an obstructive ventilatory pattern, 6 had restriction, and 12 had low KCO. In restrictive cases, KCO was reduced but remained within normal limits without compensation. The DLNO/DLCO ratio exceeded 113.5% predicted in all patients. DmCO was impaired in 7 patients, while Vc was reduced in 16.
Conclusion: Both DLCO determinants were affected, with vascular impairment predominating. Vc reduction was present in most patients, with mean values below the lower limit of normality, whereas DmCO was less affected and often normal. The elevated DLNO/DLCO ratio suggests that persistent DLCO reduction is primarily driven by prolonged pulmonary capillary circulation dysfunction rather than alveolar membrane alterations, highlighting the vascular component as the primary site of long-term impairment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


