Heemoon Park, Jung-Kyu Lee, Eun Young Heo, Deog Kyeom Kim, Hyun Woo Lee
{"title":"Maximal Forced Inspiratory Flow Dynamics and Acute Exacerbation in Chronic Obstructive Pulmonary Disease Patients with Exacerbation History.","authors":"Heemoon Park, Jung-Kyu Lee, Eun Young Heo, Deog Kyeom Kim, Hyun Woo Lee","doi":"10.4046/trd.2024.0156","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Chronic obstructive pulmonary disease (COPD), characterized by progressive airflow obstruction and frequent exacerbations, is a significant global health burden. COPD severity has traditionally been assessed using expiratory flow measurements, like forced expiratory volume in 1 second. However, the role of inspiratory flow, specifically maximal forced inspiratory flow (FIFmax), in predicting exacerbation risk is gaining attention.</p><p><strong>Methods: </strong>This retrospective cohort study evaluated COPD patients with a history of exacerbations who were receiving inhaled therapy. The eligible patients were followed up for 3 years with spirometric assessments. Patients were categorized into quartiles based on the annual change in FIFmax, from the greatest decrease (Q1) to the greatest increase (Q4). Primary outcome was acute exacerbation, stratified by severity as moderate-to-severe and severe exacerbation.</p><p><strong>Results: </strong>In total, 180 patients were followed up for 3 years. A greater increase in FIFmax was linearly associated with lower rates of both moderate-to-severe and severe exacerbations (p-value for trend <0.001 for both), but time-to-event analysis revealed no significant association between FIFmax changes and moderate-to-severe exacerbations. In contrast, a significant association with severe exacerbations was observed (log-rank p=0.005). Even after adjusting for confounders, FIFmax remained an independent predictor of severe exacerbations (Q3: hazard ratio, 0.506 [95% confidence interval, 0.306 to 0.836], p=0.008; Q4: hazard ratio, 0.491 [95% confidence interval, 0.291 to 0.830], p=0.008).</p><p><strong>Conclusion: </strong>Changes in FIFmax were not significantly associated with moderate-to-severe exacerbations, but were related to a reduced risk of severe exacerbations in COPD patients receiving inhaled therapy. These findings indicate that FIFmax may serve as a valuable prognostic marker for severe exacerbations in high-risk COPD patients.</p>","PeriodicalId":23368,"journal":{"name":"Tuberculosis and Respiratory Diseases","volume":" ","pages":"535-544"},"PeriodicalIF":3.0000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12235284/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Tuberculosis and Respiratory Diseases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4046/trd.2024.0156","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/28 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Chronic obstructive pulmonary disease (COPD), characterized by progressive airflow obstruction and frequent exacerbations, is a significant global health burden. COPD severity has traditionally been assessed using expiratory flow measurements, like forced expiratory volume in 1 second. However, the role of inspiratory flow, specifically maximal forced inspiratory flow (FIFmax), in predicting exacerbation risk is gaining attention.
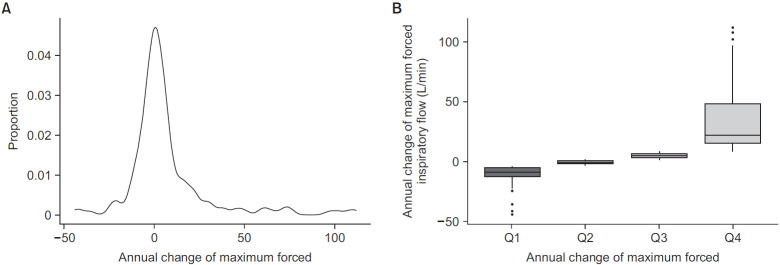
Methods: This retrospective cohort study evaluated COPD patients with a history of exacerbations who were receiving inhaled therapy. The eligible patients were followed up for 3 years with spirometric assessments. Patients were categorized into quartiles based on the annual change in FIFmax, from the greatest decrease (Q1) to the greatest increase (Q4). Primary outcome was acute exacerbation, stratified by severity as moderate-to-severe and severe exacerbation.
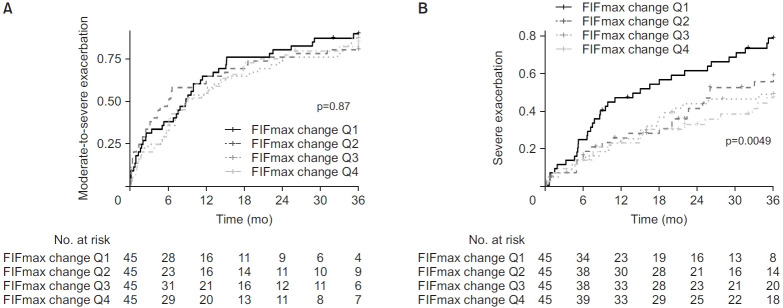
Results: In total, 180 patients were followed up for 3 years. A greater increase in FIFmax was linearly associated with lower rates of both moderate-to-severe and severe exacerbations (p-value for trend <0.001 for both), but time-to-event analysis revealed no significant association between FIFmax changes and moderate-to-severe exacerbations. In contrast, a significant association with severe exacerbations was observed (log-rank p=0.005). Even after adjusting for confounders, FIFmax remained an independent predictor of severe exacerbations (Q3: hazard ratio, 0.506 [95% confidence interval, 0.306 to 0.836], p=0.008; Q4: hazard ratio, 0.491 [95% confidence interval, 0.291 to 0.830], p=0.008).
Conclusion: Changes in FIFmax were not significantly associated with moderate-to-severe exacerbations, but were related to a reduced risk of severe exacerbations in COPD patients receiving inhaled therapy. These findings indicate that FIFmax may serve as a valuable prognostic marker for severe exacerbations in high-risk COPD patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


