Kyla L Naylor, S Joseph Kim, Bin Luo, Carol Wang, Amit X Garg, Seychelle Yohanna, Darin Treleaven, Susan McKenzie, Jane Ip, Rebecca Cooper, Nadiyah Rehman, Gregory Knoll
{"title":"Defining Referral for a Kidney Transplant Evaluation as a Quality Indicator: A Population-Based Cohort Study.","authors":"Kyla L Naylor, S Joseph Kim, Bin Luo, Carol Wang, Amit X Garg, Seychelle Yohanna, Darin Treleaven, Susan McKenzie, Jane Ip, Rebecca Cooper, Nadiyah Rehman, Gregory Knoll","doi":"10.1177/20543581251317009","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Quality indicators are required to identify gaps in care and to improve equitable access to kidney transplants. Referral to a transplant center for an evaluation is the first step toward receiving a kidney transplant, yet widespread reporting on this metric is lacking.</p><p><strong>Objective: </strong>The objective was to use administrative health care databases to examine multiple ways to define referral for a kidney transplant evaluation by varying clinical inclusion criteria, definitions for end of follow-up, and statistical methodologies.</p><p><strong>Design: </strong>This is a population-based cohort study.</p><p><strong>Setting: </strong>This study linked administrative health care databases in Ontario, Canada.</p><p><strong>Patients: </strong>Adults from Ontario, Canada, with advanced chronic kidney disease (CKD) between April 1, 2017, and March 31, 2018.</p><p><strong>Measurements: </strong>The primary outcome was the 1-year cumulative incidence of kidney transplant referral.</p><p><strong>Methods: </strong>We created several patient cohort definitions, varying patient transplant eligibility by health status (eg, whether patients had a recorded contraindication to transplant). We presented results by advanced CKD status (ie, patients approaching the need for dialysis vs receiving maintenance dialysis) and by method of cohort entry (ie, incident only vs prevalent and incident patients combined), resulting in 12 unique cohorts.</p><p><strong>Results: </strong>Sample size varied substantially from 414 to 4128 depending on the patient cohort definition, with the largest reduction in cohort size occurring when we restricted to a \"healthy\" (eg, no evidence of cardiovascular disease) group of patients. The 1-year cumulative incidence of transplant referral varied widely across cohorts. For example, in the incident maintenance dialysis population, the cumulative incidence varied more than 2-fold from 16.3% (95% confidence interval [CI] = 15.0%-17.7%) using our most inclusive cohort definition to 40.0% (95% CI = 36.0%-44.5%) using our most restrictive \"healthy\" cohort of patients.</p><p><strong>Limitations: </strong>Administrative data may have misclassified individuals' eligibility for kidney transplant.</p><p><strong>Conclusions: </strong>These results can be used by jurisdictions to measure transplant referral, a necessary step in kidney transplantation that is not equitable for all patients. Adoption of these indicators should drive quality improvement efforts that increase the number of patients referred for transplantation and ensure equitable access for all patient groups.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"12 ","pages":"20543581251317009"},"PeriodicalIF":1.5000,"publicationDate":"2025-03-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11938484/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581251317009","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Quality indicators are required to identify gaps in care and to improve equitable access to kidney transplants. Referral to a transplant center for an evaluation is the first step toward receiving a kidney transplant, yet widespread reporting on this metric is lacking.
Objective: The objective was to use administrative health care databases to examine multiple ways to define referral for a kidney transplant evaluation by varying clinical inclusion criteria, definitions for end of follow-up, and statistical methodologies.
Design: This is a population-based cohort study.
Setting: This study linked administrative health care databases in Ontario, Canada.
Patients: Adults from Ontario, Canada, with advanced chronic kidney disease (CKD) between April 1, 2017, and March 31, 2018.
Measurements: The primary outcome was the 1-year cumulative incidence of kidney transplant referral.
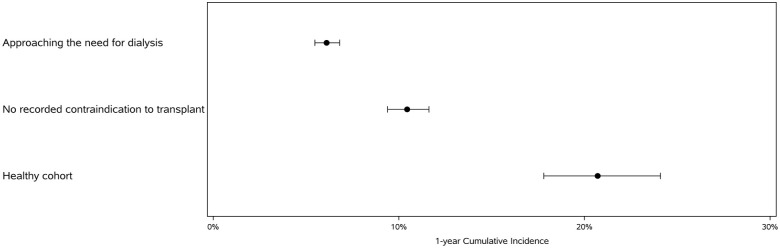
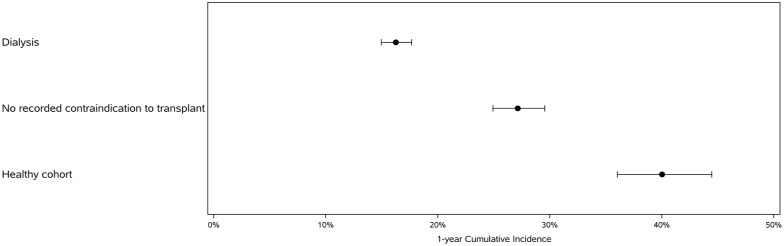
Methods: We created several patient cohort definitions, varying patient transplant eligibility by health status (eg, whether patients had a recorded contraindication to transplant). We presented results by advanced CKD status (ie, patients approaching the need for dialysis vs receiving maintenance dialysis) and by method of cohort entry (ie, incident only vs prevalent and incident patients combined), resulting in 12 unique cohorts.
Results: Sample size varied substantially from 414 to 4128 depending on the patient cohort definition, with the largest reduction in cohort size occurring when we restricted to a "healthy" (eg, no evidence of cardiovascular disease) group of patients. The 1-year cumulative incidence of transplant referral varied widely across cohorts. For example, in the incident maintenance dialysis population, the cumulative incidence varied more than 2-fold from 16.3% (95% confidence interval [CI] = 15.0%-17.7%) using our most inclusive cohort definition to 40.0% (95% CI = 36.0%-44.5%) using our most restrictive "healthy" cohort of patients.
Limitations: Administrative data may have misclassified individuals' eligibility for kidney transplant.
Conclusions: These results can be used by jurisdictions to measure transplant referral, a necessary step in kidney transplantation that is not equitable for all patients. Adoption of these indicators should drive quality improvement efforts that increase the number of patients referred for transplantation and ensure equitable access for all patient groups.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


