Mia Kassab, Abhay Katyal, Sonia Franciosi, Shubhayan Sanatani
{"title":"Chest Pain in Children: Is It Another \"Growing Pain\"?","authors":"Mia Kassab, Abhay Katyal, Sonia Franciosi, Shubhayan Sanatani","doi":"10.1002/pne2.70003","DOIUrl":null,"url":null,"abstract":"<p><p>Chest pain is a common complaint among children that has a non-cardiac origin in 99% of pediatric cases. We conducted a literature review of the different proposed etiologies of pediatric chest pain, as well as the evidence base supporting current approaches. Among the non-cardiac causes of chest pain in children, musculoskeletal causes are reported to be the most prevalent. This includes precordial catch syndrome, Tietze's syndrome, and costochondritis. However, these origins of musculoskeletal chest pain were described historically, and their labels are likely applied too broadly. It is important that providers be able to differentiate between benign chest pain that truly has a musculoskeletal origin and that which lacks an identifiable cause. To determine the cause of chest pain, providers should take a detailed history, physical examination, electrocardiogram, and any additional indicated laboratory tests. Musculoskeletal chest pain should only be diagnosed if there is an objective finding of reproducible tenderness during the physical examination or if there is a plausible history. If no cause can be identified, the chest pain may be linked to somatization. As a result, these patients may benefit from psychiatric evaluation and mindfulness-based interventions. To better inform clinical care, providers should be aware of these emerging management approaches.</p>","PeriodicalId":94166,"journal":{"name":"Paediatric & neonatal pain","volume":"7 1","pages":"e70003"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11933443/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Paediatric & neonatal pain","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/pne2.70003","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
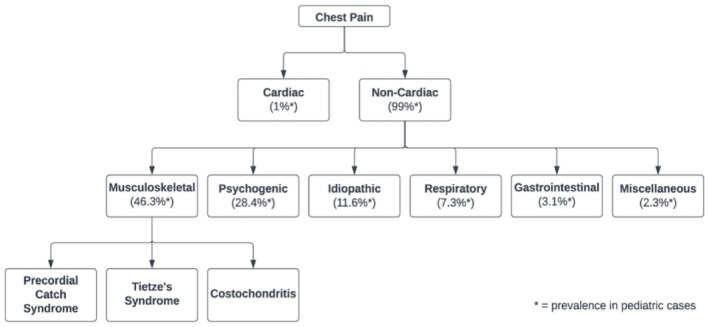
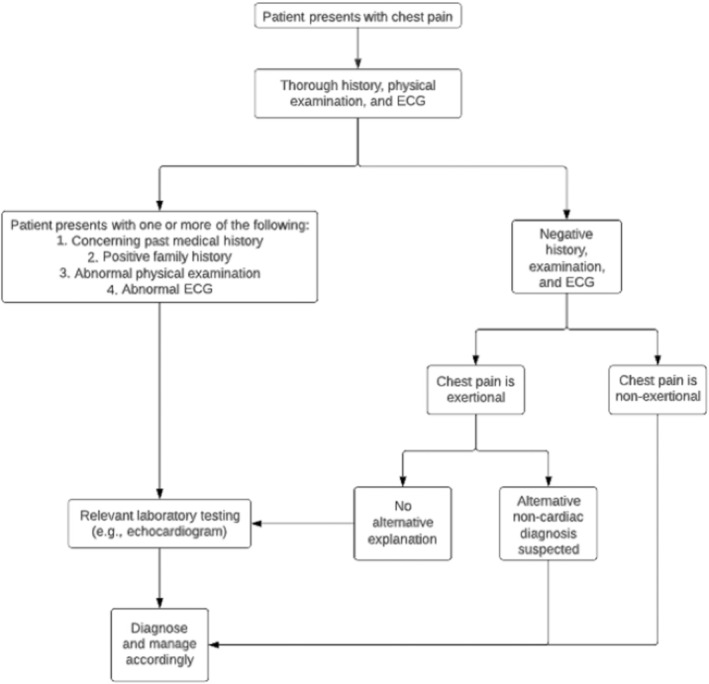
Chest pain is a common complaint among children that has a non-cardiac origin in 99% of pediatric cases. We conducted a literature review of the different proposed etiologies of pediatric chest pain, as well as the evidence base supporting current approaches. Among the non-cardiac causes of chest pain in children, musculoskeletal causes are reported to be the most prevalent. This includes precordial catch syndrome, Tietze's syndrome, and costochondritis. However, these origins of musculoskeletal chest pain were described historically, and their labels are likely applied too broadly. It is important that providers be able to differentiate between benign chest pain that truly has a musculoskeletal origin and that which lacks an identifiable cause. To determine the cause of chest pain, providers should take a detailed history, physical examination, electrocardiogram, and any additional indicated laboratory tests. Musculoskeletal chest pain should only be diagnosed if there is an objective finding of reproducible tenderness during the physical examination or if there is a plausible history. If no cause can be identified, the chest pain may be linked to somatization. As a result, these patients may benefit from psychiatric evaluation and mindfulness-based interventions. To better inform clinical care, providers should be aware of these emerging management approaches.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


