{"title":"Transition from acute kidney injury to chronic kidney disease in liver cirrhosis patients: Current perspective.","authors":"Sudheer Marrapu, Ramesh Kumar","doi":"10.5527/wjn.v14.i1.102381","DOIUrl":null,"url":null,"abstract":"<p><p>In liver cirrhosis patients, acute kidney injury (AKI) is a common and severe complication associated with significant morbidity and mortality, often leading to chronic kidney disease (CKD). This progression reflects a complex interplay of renal and hepatic pathophysiology, with AKI acting as an initiator through maladaptive repair mechanisms. These mechanisms-such as tubular cell cycle arrest, inflammatory cascades, and fibrotic processes-are exacerbated by the hemodynamic and neurohormonal disturbances characteristic of cirrhosis. Following AKI episodes, persistent kidney dysfunction or acute kidney disease (AKD) often serves as a bridge to CKD. AKD represents a critical phase in renal deterioration, characterized by prolonged kidney injury that does not fully meet CKD criteria but exceeds the temporal scope of AKI. The progression from AKD to CKD is further influenced by recurrent AKI episodes, impaired renal autoregulation, and systemic comorbidities such as diabetes and metabolic dysfunction-associated steatotic liver disease, which compound kidney damage. The clinical management of AKI and CKD in cirrhotic patients requires a multidimensional approach that includes early identification of kidney injury, the application of novel biomarkers, and precision interventions. Recent evidence underscores the inadequacy of traditional biomarkers in predicting the AKI-to-CKD progression, necessitating novel biomarkers for early detection and intervention.</p>","PeriodicalId":94272,"journal":{"name":"World journal of nephrology","volume":"14 1","pages":"102381"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11755238/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World journal of nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5527/wjn.v14.i1.102381","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
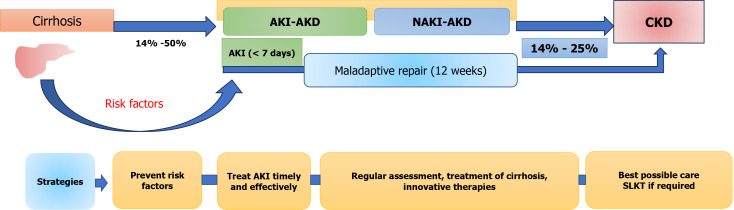
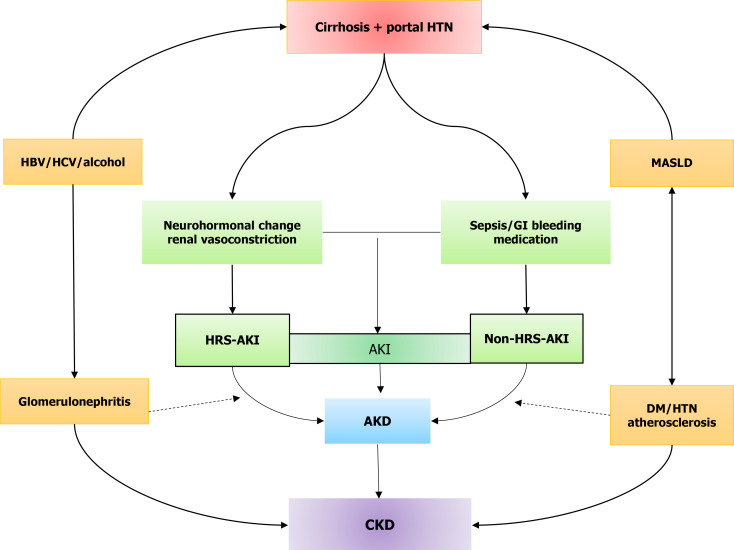
In liver cirrhosis patients, acute kidney injury (AKI) is a common and severe complication associated with significant morbidity and mortality, often leading to chronic kidney disease (CKD). This progression reflects a complex interplay of renal and hepatic pathophysiology, with AKI acting as an initiator through maladaptive repair mechanisms. These mechanisms-such as tubular cell cycle arrest, inflammatory cascades, and fibrotic processes-are exacerbated by the hemodynamic and neurohormonal disturbances characteristic of cirrhosis. Following AKI episodes, persistent kidney dysfunction or acute kidney disease (AKD) often serves as a bridge to CKD. AKD represents a critical phase in renal deterioration, characterized by prolonged kidney injury that does not fully meet CKD criteria but exceeds the temporal scope of AKI. The progression from AKD to CKD is further influenced by recurrent AKI episodes, impaired renal autoregulation, and systemic comorbidities such as diabetes and metabolic dysfunction-associated steatotic liver disease, which compound kidney damage. The clinical management of AKI and CKD in cirrhotic patients requires a multidimensional approach that includes early identification of kidney injury, the application of novel biomarkers, and precision interventions. Recent evidence underscores the inadequacy of traditional biomarkers in predicting the AKI-to-CKD progression, necessitating novel biomarkers for early detection and intervention.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


