Chih-Yuan Lin, Chih-Ching Liu, Yu-Tung Huang, Yue-Chune Lee
{"title":"Policy Spotlight Effects on Critical Time-Sensitive Diseases: Nationwide Retrospective Cohort Study on Taiwan's Hospital Emergency Capability Categorization Policy.","authors":"Chih-Yuan Lin, Chih-Ching Liu, Yu-Tung Huang, Yue-Chune Lee","doi":"10.2196/54651","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Taiwan's categorization of hospital emergency capability (CHEC) policy is designed to regionalize and dispatch critical patients. The policy was designed in 2009 to improve the quality of emergency care for critical time-sensitive diseases (CTSDs). The CHEC policy primarily uses time-based quality surveillance indicators.</p><p><strong>Objective: </strong>We aimed to investigate the impact of Taiwan's CHEC policy on CTSDs.</p><p><strong>Methods: </strong>Using Taiwan's 2005 Longitudinal Health Insurance Database, this nationwide retrospective cohort study examined the CHEC policy's impact from 2005 to 2011. Propensity score matching and difference-in-differences analysis within a generalized estimating equation framework were used to compare pre- and postimplementation periods. The study focused on acute ischemic stroke (AIS), ST-segment elevation myocardial infarction (STEMI), septic shock, and major trauma. AIS and STEMI cases, monitored with time-based indicators, were evaluated for adherence to diagnostic and treatment guidelines as process quality measures. Mortality and medical use served as outcome indicators. Major trauma, with evolving guidelines and no time-based monitoring, acted as a control to test for policy spotlight effects.</p><p><strong>Results: </strong>In our cohort of 9923 patients, refined through 1:1 propensity score matching, 5566 (56.09%) were male and were mostly older adults. Our analysis revealed that the CHEC policy effectively improved system efficiency and patient outcomes, resulting in significant reductions in medical orders (-7.29 items, 95% CI -10.09 to -4.48; P<.001), short-term mortality rates (-0.09%, 95% CI -0.17% to -0.02%; P=.01) and long-term mortality rates (-0.09%, 95% CI -0.15% to -0.04%; P=.001), and total medical expenses (-5328.35 points per case, 95% CI -10,387.10 to -269.60; P=.04), despite a modest increase in diagnostic fees (376.37 points, 95% CI 92.42-660.33; P=.01). The CHEC policy led to notable increases in diagnostic fees, major treatments, and medical orders for AIS and STEMI cases. For AIS cases, significant increases were observed in major treatments (β=0.77; 95% CI 0.21-1.33; P=.007) and medical orders (β=15.20; 95% CI 5.28-25.11; P=.003) compared to major trauma. In STEMI cases, diagnostic fees significantly increased (β=1983.75; 95% CI 84.28-3883.21; P=.04), while upward transfer rates significantly decreased (β=-0.59; 95% CI -1.18 to -0.001; P=.049). There were also trends toward increased major treatments (β=0.30; 95% CI -0.03 to 0.62, P=.07), medical orders (β=11.92; 95% CI -0.90 to 24.73; P=.07), and medical expenses (β=24,275.54; 95% CI -640.71 to 4,991,991.78; P=.06), although these were not statistically significant. In contrast, no significant changes were identified in process or outcome quality indicators for septic shock. These findings suggest policy spotlight effects, reflecting a greater emphasis on diseases directly prioritized under the CHEC policy.</p><p><strong>Conclusions: </strong>The CHEC policy demonstrated the dual benefits of reducing costs and improving patient outcomes. We observed unintended consequences of policy spotlight effects, which led to a disproportionate improvement in guideline adherence and process quality for CTSDs with time-based surveillance indicators.</p>","PeriodicalId":51757,"journal":{"name":"Interactive Journal of Medical Research","volume":"14 ","pages":"e54651"},"PeriodicalIF":1.9000,"publicationDate":"2025-03-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11979550/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interactive Journal of Medical Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/54651","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Taiwan's categorization of hospital emergency capability (CHEC) policy is designed to regionalize and dispatch critical patients. The policy was designed in 2009 to improve the quality of emergency care for critical time-sensitive diseases (CTSDs). The CHEC policy primarily uses time-based quality surveillance indicators.
Objective: We aimed to investigate the impact of Taiwan's CHEC policy on CTSDs.
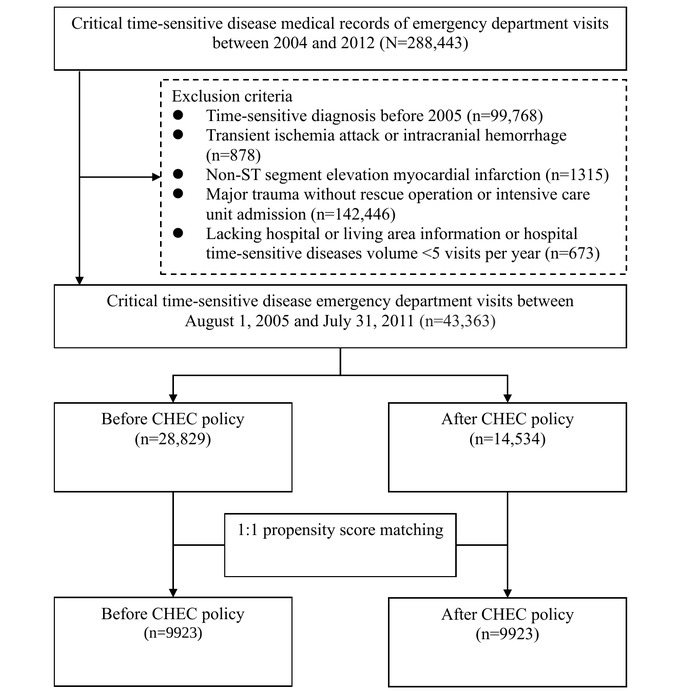
Methods: Using Taiwan's 2005 Longitudinal Health Insurance Database, this nationwide retrospective cohort study examined the CHEC policy's impact from 2005 to 2011. Propensity score matching and difference-in-differences analysis within a generalized estimating equation framework were used to compare pre- and postimplementation periods. The study focused on acute ischemic stroke (AIS), ST-segment elevation myocardial infarction (STEMI), septic shock, and major trauma. AIS and STEMI cases, monitored with time-based indicators, were evaluated for adherence to diagnostic and treatment guidelines as process quality measures. Mortality and medical use served as outcome indicators. Major trauma, with evolving guidelines and no time-based monitoring, acted as a control to test for policy spotlight effects.
Results: In our cohort of 9923 patients, refined through 1:1 propensity score matching, 5566 (56.09%) were male and were mostly older adults. Our analysis revealed that the CHEC policy effectively improved system efficiency and patient outcomes, resulting in significant reductions in medical orders (-7.29 items, 95% CI -10.09 to -4.48; P<.001), short-term mortality rates (-0.09%, 95% CI -0.17% to -0.02%; P=.01) and long-term mortality rates (-0.09%, 95% CI -0.15% to -0.04%; P=.001), and total medical expenses (-5328.35 points per case, 95% CI -10,387.10 to -269.60; P=.04), despite a modest increase in diagnostic fees (376.37 points, 95% CI 92.42-660.33; P=.01). The CHEC policy led to notable increases in diagnostic fees, major treatments, and medical orders for AIS and STEMI cases. For AIS cases, significant increases were observed in major treatments (β=0.77; 95% CI 0.21-1.33; P=.007) and medical orders (β=15.20; 95% CI 5.28-25.11; P=.003) compared to major trauma. In STEMI cases, diagnostic fees significantly increased (β=1983.75; 95% CI 84.28-3883.21; P=.04), while upward transfer rates significantly decreased (β=-0.59; 95% CI -1.18 to -0.001; P=.049). There were also trends toward increased major treatments (β=0.30; 95% CI -0.03 to 0.62, P=.07), medical orders (β=11.92; 95% CI -0.90 to 24.73; P=.07), and medical expenses (β=24,275.54; 95% CI -640.71 to 4,991,991.78; P=.06), although these were not statistically significant. In contrast, no significant changes were identified in process or outcome quality indicators for septic shock. These findings suggest policy spotlight effects, reflecting a greater emphasis on diseases directly prioritized under the CHEC policy.
Conclusions: The CHEC policy demonstrated the dual benefits of reducing costs and improving patient outcomes. We observed unintended consequences of policy spotlight effects, which led to a disproportionate improvement in guideline adherence and process quality for CTSDs with time-based surveillance indicators.
背景:台湾的医院急救能力分类政策是为了区分和分派危重病人。这项政策是2009年制定的,目的是提高对严重时效性疾病的急诊护理质量。CHEC政策主要使用基于时间的质量监控指标。目的:探讨中国台湾地区CHEC政策对CTSDs的影响。方法:利用台湾2005年健康保险纵向数据库,对2005年至2011年健康保险政策的影响进行回顾性队列研究。在广义估计方程框架内使用倾向得分匹配和差异中差异分析来比较实施前后的时期。该研究的重点是急性缺血性卒中(AIS)、st段抬高型心肌梗死(STEMI)、感染性休克和重大创伤。AIS和STEMI病例采用基于时间的指标进行监测,作为过程质量措施,评估其对诊断和治疗指南的依从性。死亡率和医疗使用作为结果指标。重大创伤的指导方针不断发展,没有基于时间的监测,作为测试政策聚光灯效应的对照。结果:在我们的9923例患者队列中,通过1:1倾向评分匹配细化,5566例(56.09%)为男性,大多数为老年人。我们的分析显示,CHEC政策有效地提高了系统效率和患者预后,导致医疗订单显著减少(-7.29项,95% CI -10.09至-4.48;结论:CHEC政策显示了降低成本和改善患者预后的双重益处。我们观察到政策聚光灯效应的意想不到的后果,这导致具有基于时间的监测指标的ctsd的指南依从性和过程质量的不成比例的改善。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


