Assessment of mortality due to severe SARS-CoV-2 infection in public and private intensive care units in Brazil: a multicenter retrospective cohort study.
Thiago Domingos Corrêa, Thais Dias Midega, Ricardo Kenji Nawa, Ricardo Luiz Cordioli, Adriano José Pereira, Moacyr Silva Júnior, Bruno de Arruda Bravim, Niklas Soderberg Campos, Amanda Pascoal Valle Felicio, Angelo Antônio Gomes de Carvalho, Andreia Pardini, Raquel Afonso Caserta Eid, Rodrigo Dias Rodrigues, Marcele Liliane Pesavento, Leonardo Van de Wiel Barros Urbano Andari, Bento Fortunato Cardoso Dos Santos, Claudia Regina Laselva, Felipe Maia de Toledo Piza, Miguel Cendoroglo Neto, Guilherme de Paula Pinto Schettino, Sidney Klajner, Leonardo José Rolim Ferraz
{"title":"Assessment of mortality due to severe SARS-CoV-2 infection in public and private intensive care units in Brazil: a multicenter retrospective cohort study.","authors":"Thiago Domingos Corrêa, Thais Dias Midega, Ricardo Kenji Nawa, Ricardo Luiz Cordioli, Adriano José Pereira, Moacyr Silva Júnior, Bruno de Arruda Bravim, Niklas Soderberg Campos, Amanda Pascoal Valle Felicio, Angelo Antônio Gomes de Carvalho, Andreia Pardini, Raquel Afonso Caserta Eid, Rodrigo Dias Rodrigues, Marcele Liliane Pesavento, Leonardo Van de Wiel Barros Urbano Andari, Bento Fortunato Cardoso Dos Santos, Claudia Regina Laselva, Felipe Maia de Toledo Piza, Miguel Cendoroglo Neto, Guilherme de Paula Pinto Schettino, Sidney Klajner, Leonardo José Rolim Ferraz","doi":"10.31744/einstein_journal/2025AO1060","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This retrospective multicenter cohort study compared characteristics and outcomes of 5,790 critically ill patients with COVID-19 in Brazil's public and private intensive care units. Patients in public intensive care units exhibited greater disease severity, more frequent use of organ support, and higher mortality rates compared to those in private intensive care units. The risk of in-hospital death was more than twice as high in public intensive care units. ■ Public intensive care unit COVID-19 patients presented with more comorbidities and higher severity at admission. ■ Public intensive care units required more invasive organ support (e.g., mechanical ventilation, vasopressors, and renal replacement therapy) but less non-invasive ventilation and high-flow nasal cannula than private intensive care units. ■ In-hospital mortality was higher in public intensive care units, with an increased risk of death even after adjusting for patient characteristics and illness severity at intensive care unit admission.</p><p><strong>Objective: </strong>To compare the clinical characteristics, use of organ support, and outcomes of critically ill patients with COVID-19 admitted to public and private intensive care units.</p><p><strong>Methods: </strong>This multicenter retrospective cohort study included patients admitted to four intensive care units from March 1, 2020, to December 31, 2021. Patients with COVID-19 admitted to public and private intensive care units were compared. The primary outcome of interest, in-hospital mortality, was assessed using a hierarchical logistic regression (multilevel) model adjusted for study site and patient characteristics.</p><p><strong>Results: </strong>A total of 5,790 patients with COVID-19 were admitted to the participating intensive care units, with 3,321 (57.3%) admitted to private hospitals and 2,469 (42.6%) admitted to public hospitals. Patients in public intensive care units were less likely to be male and had higher median SAPS III scores, Charlson Comorbidity Index values, and SOFA scores. They also required mechanical ventilation (53.1% versus 40.0%, p<0.001), vasopressors (43.1% versus 33.9%, p<0.001), and renal replacement therapy (20.3% versus. 14.5%, p<0.001) more frequently than those in private intensive care units. In contrast, patients in private intensive care units were more frequently managed with non-invasive ventilation (38.0% versus 66.8%; p<0.001) and high-flow nasal cannulas (18.3% versus 48.1%; p<0.001). The in-hospital mortality rate was significantly higher in public intensive care units (40.3%) compared to private intensive care units (16.4%) (adjusted OR=2.96; 95%CI=1.94-4.51; p<0.001).</p><p><strong>Conclusion: </strong>We observed significant differences in resource utilization and mortality rates between patients with COVID-19 admitted to public and private intensive care units. Patients with COVID-19 in public care units face a higher risk of in-hospital mortality compared to those in private care units.</p>","PeriodicalId":47359,"journal":{"name":"Einstein-Sao Paulo","volume":"23 spe1","pages":"eAO1060"},"PeriodicalIF":0.9000,"publicationDate":"2025-03-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11999376/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Einstein-Sao Paulo","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31744/einstein_journal/2025AO1060","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: This retrospective multicenter cohort study compared characteristics and outcomes of 5,790 critically ill patients with COVID-19 in Brazil's public and private intensive care units. Patients in public intensive care units exhibited greater disease severity, more frequent use of organ support, and higher mortality rates compared to those in private intensive care units. The risk of in-hospital death was more than twice as high in public intensive care units. ■ Public intensive care unit COVID-19 patients presented with more comorbidities and higher severity at admission. ■ Public intensive care units required more invasive organ support (e.g., mechanical ventilation, vasopressors, and renal replacement therapy) but less non-invasive ventilation and high-flow nasal cannula than private intensive care units. ■ In-hospital mortality was higher in public intensive care units, with an increased risk of death even after adjusting for patient characteristics and illness severity at intensive care unit admission.
Objective: To compare the clinical characteristics, use of organ support, and outcomes of critically ill patients with COVID-19 admitted to public and private intensive care units.
Methods: This multicenter retrospective cohort study included patients admitted to four intensive care units from March 1, 2020, to December 31, 2021. Patients with COVID-19 admitted to public and private intensive care units were compared. The primary outcome of interest, in-hospital mortality, was assessed using a hierarchical logistic regression (multilevel) model adjusted for study site and patient characteristics.
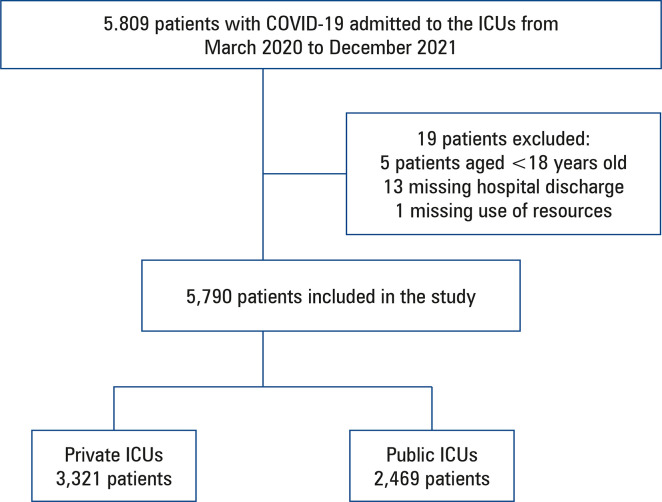
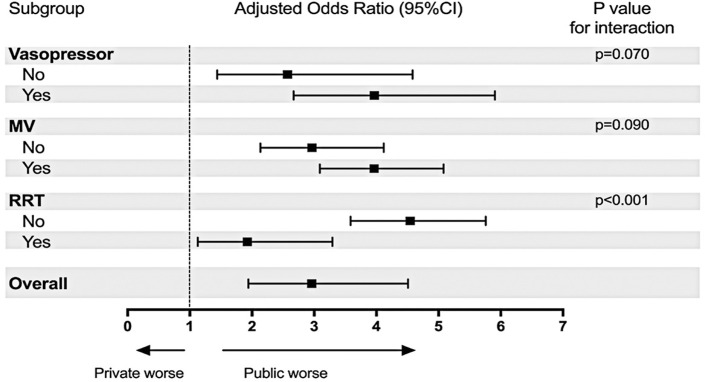
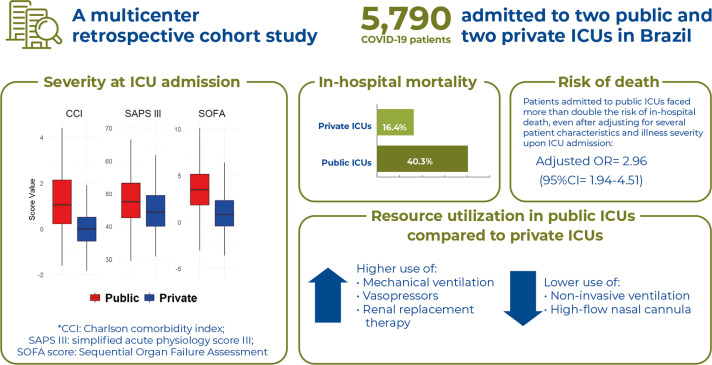
Results: A total of 5,790 patients with COVID-19 were admitted to the participating intensive care units, with 3,321 (57.3%) admitted to private hospitals and 2,469 (42.6%) admitted to public hospitals. Patients in public intensive care units were less likely to be male and had higher median SAPS III scores, Charlson Comorbidity Index values, and SOFA scores. They also required mechanical ventilation (53.1% versus 40.0%, p<0.001), vasopressors (43.1% versus 33.9%, p<0.001), and renal replacement therapy (20.3% versus. 14.5%, p<0.001) more frequently than those in private intensive care units. In contrast, patients in private intensive care units were more frequently managed with non-invasive ventilation (38.0% versus 66.8%; p<0.001) and high-flow nasal cannulas (18.3% versus 48.1%; p<0.001). The in-hospital mortality rate was significantly higher in public intensive care units (40.3%) compared to private intensive care units (16.4%) (adjusted OR=2.96; 95%CI=1.94-4.51; p<0.001).
Conclusion: We observed significant differences in resource utilization and mortality rates between patients with COVID-19 admitted to public and private intensive care units. Patients with COVID-19 in public care units face a higher risk of in-hospital mortality compared to those in private care units.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


