Breanna J. Teleki BND Hons, Elizabeth Viner Smith PhD, Rosalie Yandell PhD, Matthew J. Summers MDiet, Lee-anne S. Chapple PhD
{"title":"Nutrition-impacting symptoms in survivors of critical illness: A descriptive cohort study","authors":"Breanna J. Teleki BND Hons, Elizabeth Viner Smith PhD, Rosalie Yandell PhD, Matthew J. Summers MDiet, Lee-anne S. Chapple PhD","doi":"10.1002/jpen.2753","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Oral intake is the most common route of nutrition following intensive care unit (ICU) discharge; yet is associated with inadequate intake, and barriers are largely unknown. This study aimed to determine the prevalence and severity of symptoms that may impact oral intake (termed nutrition-impacting symptoms) in ICU survivors.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>A single-center descriptive cohort study quantified prevalence and severity of nutrition-impacting symptoms in ICU survivors at ICU (T1) and hospital (T2) discharge and at 1 month posthospital discharge (T3) via patient-reported questionnaires. Secondary outcomes were nutrition status (via Subjective Global Assessment) and energy and protein intakes (via 24-h recall). Data are median (IQR) or (percent).</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Forty-nine ICU survivors (64 [51–71] years; 31% female) were included. The most prevalent nutrition-impacting symptoms were T1: tiredness (96%), loss of appetite (82%), and early satiety (82%); T2: tiredness (93%), early satiety (88%), and dry mouth (78%); and T3: tiredness (95%), early satiety (81%), and low mood (66%). Nutrition-impacting symptoms with the greatest severity (out of 10, higher equates to worse) at each time point were T1: tiredness, constipation, diarrhea, nausea (all 8 [5–10]); T2: tiredness and constipation (both 7 [5–8]); and T3: tiredness (6 [3–8]) and diarrhea (6 [2–7]). Malnutrition rates were 34% at T1. Energy and protein intakes were T1: 1046 [548–1481] kcal, 45.2 [23.9–61.0] g; T2: 1370 [958–1962] kcal, 70.9 [39.0–92.2] g; T3: 1580 [1168–2042] kcal, 45.2 [54.6–100.4] g.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>ICU survivors experience multiple nutrition-impacting symptoms of varying prevalence and severity, which improve across the post-ICU continuum.</p>\n </section>\n </div>","PeriodicalId":16668,"journal":{"name":"Journal of Parenteral and Enteral Nutrition","volume":"49 6","pages":"742-751"},"PeriodicalIF":4.1000,"publicationDate":"2025-03-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jpen.2753","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Parenteral and Enteral Nutrition","FirstCategoryId":"3","ListUrlMain":"https://aspenjournals.onlinelibrary.wiley.com/doi/10.1002/jpen.2753","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"NUTRITION & DIETETICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Oral intake is the most common route of nutrition following intensive care unit (ICU) discharge; yet is associated with inadequate intake, and barriers are largely unknown. This study aimed to determine the prevalence and severity of symptoms that may impact oral intake (termed nutrition-impacting symptoms) in ICU survivors.
Methods
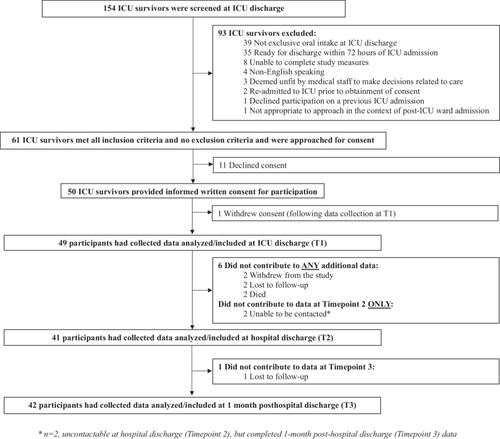
A single-center descriptive cohort study quantified prevalence and severity of nutrition-impacting symptoms in ICU survivors at ICU (T1) and hospital (T2) discharge and at 1 month posthospital discharge (T3) via patient-reported questionnaires. Secondary outcomes were nutrition status (via Subjective Global Assessment) and energy and protein intakes (via 24-h recall). Data are median (IQR) or (percent).
Results
Forty-nine ICU survivors (64 [51–71] years; 31% female) were included. The most prevalent nutrition-impacting symptoms were T1: tiredness (96%), loss of appetite (82%), and early satiety (82%); T2: tiredness (93%), early satiety (88%), and dry mouth (78%); and T3: tiredness (95%), early satiety (81%), and low mood (66%). Nutrition-impacting symptoms with the greatest severity (out of 10, higher equates to worse) at each time point were T1: tiredness, constipation, diarrhea, nausea (all 8 [5–10]); T2: tiredness and constipation (both 7 [5–8]); and T3: tiredness (6 [3–8]) and diarrhea (6 [2–7]). Malnutrition rates were 34% at T1. Energy and protein intakes were T1: 1046 [548–1481] kcal, 45.2 [23.9–61.0] g; T2: 1370 [958–1962] kcal, 70.9 [39.0–92.2] g; T3: 1580 [1168–2042] kcal, 45.2 [54.6–100.4] g.
Conclusions
ICU survivors experience multiple nutrition-impacting symptoms of varying prevalence and severity, which improve across the post-ICU continuum.
期刊介绍:
The Journal of Parenteral and Enteral Nutrition (JPEN) is the premier scientific journal of nutrition and metabolic support. It publishes original peer-reviewed studies that define the cutting edge of basic and clinical research in the field. It explores the science of optimizing the care of patients receiving enteral or IV therapies. Also included: reviews, techniques, brief reports, case reports, and abstracts.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


