Comparison of outcomes between pulsatile gonadotropin releasing hormone and combined gonadotropin therapy of spermatogenesis in patients with congenital hypogonadotropic hypogonadism.
Yi Zheng, Heng-Zhou Bai, Gui-Cheng Zhao, Kun Tian, Jun-Tao Yue, Ding-Ming Li, Xiao-Hui Jiang
{"title":"Comparison of outcomes between pulsatile gonadotropin releasing hormone and combined gonadotropin therapy of spermatogenesis in patients with congenital hypogonadotropic hypogonadism.","authors":"Yi Zheng, Heng-Zhou Bai, Gui-Cheng Zhao, Kun Tian, Jun-Tao Yue, Ding-Ming Li, Xiao-Hui Jiang","doi":"10.1186/s12958-025-01370-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>To evaluate whether there was a difference in outcome between pulsatile gonadotropin releasing hormone (GnRH) therapy and human chorionic gonadotropin/human menopausal gonadotropin (hCG/HMG) therapy for induction of spermatogenesis in post-pubertal male patients with congenital hypogonadotropic hypogonadism (CHH).</p><p><strong>Methods: </strong>This was a single-center retrospective cohort study conducted at the Andrology Center of a university hospital. A total of 155 postpubertal CHH patients who met the inclusion criteria underwent spermatogenic induction at the same andrology center. All patients used pulsatile GnRH therapy or hCG/HMG therapy for at least 6 months. The effects of spermatogenic induction therapy and testicular growth were evaluated. Logistic regression analysis was used to identify statistically significant factors which could predict the outcome of treatment.</p><p><strong>Results: </strong>There was no difference in the efficiency of successfully inducing spermatogenesis between pulsatile GnRH therapy and hCG/HMG therapy (82.1% vs. 75.8%, P: 0.356), nor was there a difference in sperm concentration category (SCC) (P: 0.284). However, the mean time required for pulsatile GnRH therapy was shorter (12.34 vs. 14.74 months, P: 0.038). At the treatment endpoint, total testicular volume (TTV) was greater with pulsatile GnRH therapy compared with hCG/HMG therapy (15 vs. 12 ml, P: 0.010), and there was still no difference in SCC (P: 0.310). Multivariate logistic regression analysis showed that only baseline TTV was statistically significant predictor of induced spermatogenic success (odds ratio, OR: 1.156, 95% confidence interval, CI: 1.013, 1.319). The area under receiver operating characteristic curve was 0.635, a sensitivity of 0.661, and a specificity of 0.588. In addition, multiple linear regression analysis demonstrated that younger age at treatment initiation and higher baseline TTV were significantly associated with increased sperm concentration at the end of treatment.</p><p><strong>Conclusion: </strong>Pulsatile GnRH therapy was similar to hCG/HMG therapy in inducing spermatogenesis in post-pubertal CHH patients, but it took less time and was more beneficial to testicular development. Larger baseline TTV may mean a better spermatogenic outcome. It was necessary for patients to have more information about spermatogenesis therapy in order to make reasonable medical decisions.</p><p><strong>Clinical trial registration number: </strong>Chinese Clinical Trial Registry. ChiCTR2400086876. Retrospectively registered on July 5, 2024.</p>","PeriodicalId":21011,"journal":{"name":"Reproductive Biology and Endocrinology","volume":"23 1","pages":"46"},"PeriodicalIF":4.7000,"publicationDate":"2025-03-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11927256/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Reproductive Biology and Endocrinology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12958-025-01370-7","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: To evaluate whether there was a difference in outcome between pulsatile gonadotropin releasing hormone (GnRH) therapy and human chorionic gonadotropin/human menopausal gonadotropin (hCG/HMG) therapy for induction of spermatogenesis in post-pubertal male patients with congenital hypogonadotropic hypogonadism (CHH).
Methods: This was a single-center retrospective cohort study conducted at the Andrology Center of a university hospital. A total of 155 postpubertal CHH patients who met the inclusion criteria underwent spermatogenic induction at the same andrology center. All patients used pulsatile GnRH therapy or hCG/HMG therapy for at least 6 months. The effects of spermatogenic induction therapy and testicular growth were evaluated. Logistic regression analysis was used to identify statistically significant factors which could predict the outcome of treatment.
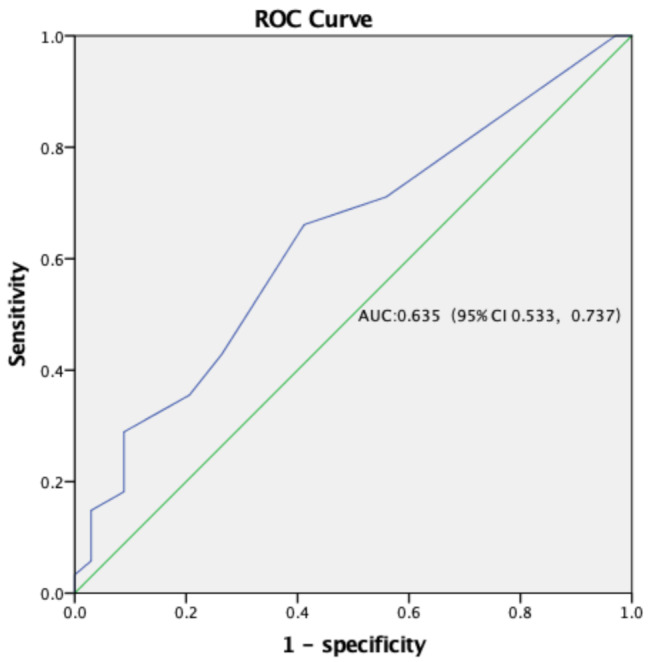
Results: There was no difference in the efficiency of successfully inducing spermatogenesis between pulsatile GnRH therapy and hCG/HMG therapy (82.1% vs. 75.8%, P: 0.356), nor was there a difference in sperm concentration category (SCC) (P: 0.284). However, the mean time required for pulsatile GnRH therapy was shorter (12.34 vs. 14.74 months, P: 0.038). At the treatment endpoint, total testicular volume (TTV) was greater with pulsatile GnRH therapy compared with hCG/HMG therapy (15 vs. 12 ml, P: 0.010), and there was still no difference in SCC (P: 0.310). Multivariate logistic regression analysis showed that only baseline TTV was statistically significant predictor of induced spermatogenic success (odds ratio, OR: 1.156, 95% confidence interval, CI: 1.013, 1.319). The area under receiver operating characteristic curve was 0.635, a sensitivity of 0.661, and a specificity of 0.588. In addition, multiple linear regression analysis demonstrated that younger age at treatment initiation and higher baseline TTV were significantly associated with increased sperm concentration at the end of treatment.
Conclusion: Pulsatile GnRH therapy was similar to hCG/HMG therapy in inducing spermatogenesis in post-pubertal CHH patients, but it took less time and was more beneficial to testicular development. Larger baseline TTV may mean a better spermatogenic outcome. It was necessary for patients to have more information about spermatogenesis therapy in order to make reasonable medical decisions.
Clinical trial registration number: Chinese Clinical Trial Registry. ChiCTR2400086876. Retrospectively registered on July 5, 2024.
期刊介绍:
Reproductive Biology and Endocrinology publishes and disseminates high-quality results from excellent research in the reproductive sciences.
The journal publishes on topics covering gametogenesis, fertilization, early embryonic development, embryo-uterus interaction, reproductive development, pregnancy, uterine biology, endocrinology of reproduction, control of reproduction, reproductive immunology, neuroendocrinology, and veterinary and human reproductive medicine, including all vertebrate species.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


