Twelve-year trends of hospitalizations and survival of acute decompensated heart failure: Data from a regional tertiary center
IF 2.6
3区 医学
Q2 CARDIAC & CARDIOVASCULAR SYSTEMS
引用次数: 0
Abstract
Background
Recent trends in in-hospital acute decompensated heart failure (ADHF) have been reported in several registry studies demonstrating no improvement in terms of mortality rate and readmission rate due to heart failure (HF) exacerbation. Trends in management of ADHF may be different in areas where the aging rate is faster.
Methods
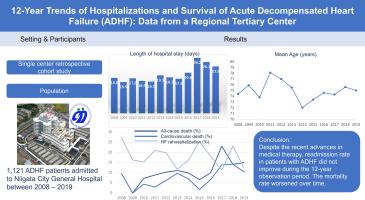
We retrospectively enrolled 1121 ADHF patients hospitalized between 2008 and 2019. The study patients were classified into three groups based on 4-year periods. Our primary study interests were trends over time in age, length of hospital stay, and clinical outcomes, with endpoints, including 1-year mortality and readmission for HF (reHF).
Results
During the 12-year period, the length of hospital stay was not reduced, but rather prolonged in Period 3 (p < 0.001). Temporal trends in 1-year clinical outcomes showed both 1-year all-cause and cardiovascular mortality tended to increase. No improvement in 1-year reHF rates was observed over time. All-cause mortality was associated with Period 2 (95%CI 1.02–4.97), Period 3 (95%CI 1.30–6.05), older age (≥79 years, 95%CI 1.01–3.20), decreased left ventricular ejection fraction (95%CI 1.08–3.62), higher loop diuretics dose (95%CI 1.07–1.25), higher B-type natriuretic peptide (BNP) levels (95%CI 1.00, 1.01), and decreased hemoglobin levels (95%CI 0.74–0.97). Factors associated with cardiovascular mortality included Period 3 (95%CI 1.02–7.31), higher loop diuretics dose (HR 1.17, 95%CI 1.07–1.27), higher BNP levels (95%CI1.00–1.01), and lower estimated glomerular filtration rate (eGFR) levels on admission (95%CI 0.70–0.95). Predictors of reHF were number of previous HF hospitalizations (95%CI 1.13–1.94), lower eGFR levels (95%CI 0.79–0.94) on admission and suboptimal guideline-directed medical therapy (95%CI 0.50–0.79).
Conclusions
Despite the recent advances in medical therapy, readmission rate in patients with ADHF did not improve during the 12-year observation period. The mortality rate worsened over time. These findings warrant prompt establishment of more effective approaches to prevent and treat ADHF.
急性失代偿性心力衰竭的住院和生存的12年趋势:来自区域三级中心的数据。
背景:近期住院急性失代偿性心力衰竭(ADHF)的趋势已经在几项登记研究中报道,表明由于心力衰竭(HF)恶化导致的死亡率和再入院率没有改善。在老龄化速度较快的地区,ADHF的管理趋势可能有所不同。方法:回顾性纳入2008年至2019年间住院的1121例ADHF患者。研究患者以4年为周期分为三组。我们的主要研究兴趣是年龄、住院时间和临床结果的趋势,终点包括1年死亡率和HF再入院(reHF)。结果:在12年的观察期内,ADHF患者的住院时间非但没有减少,反而延长了(p )。结论:尽管近年来药物治疗取得了进展,但在12年的观察期内,ADHF患者的再入院率并没有提高。死亡率随着时间的推移而恶化。这些发现要求迅速建立更有效的方法来预防和治疗ADHF。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊
Journal of cardiology
CARDIAC & CARDIOVASCULAR SYSTEMS-
CiteScore
4.90
自引率
8.00%
发文量
202
审稿时长
29 days
期刊介绍:
The official journal of the Japanese College of Cardiology is an international, English language, peer-reviewed journal publishing the latest findings in cardiovascular medicine. Journal of Cardiology (JC) aims to publish the highest-quality material covering original basic and clinical research on all aspects of cardiovascular disease. Topics covered include ischemic heart disease, cardiomyopathy, valvular heart disease, vascular disease, hypertension, arrhythmia, congenital heart disease, pharmacological and non-pharmacological treatment, new diagnostic techniques, and cardiovascular imaging. JC also publishes a selection of review articles, clinical trials, short communications, and important messages and letters to the editor.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


