Digital health programme following rhythm control in patients with atrial fibrillation: comprehensive disease management by self-monitoring, coaching, and telemedicine.
Georges von Degenfeld, Anke Langbein, Alessandra Boscheri, Maximilian O Ziegler, Jonas Demlehner, Paul Weyh, Alexander Leber, Sandra Schreier, Stefan G Spitzer
{"title":"Digital health programme following rhythm control in patients with atrial fibrillation: comprehensive disease management by self-monitoring, coaching, and telemedicine.","authors":"Georges von Degenfeld, Anke Langbein, Alessandra Boscheri, Maximilian O Ziegler, Jonas Demlehner, Paul Weyh, Alexander Leber, Sandra Schreier, Stefan G Spitzer","doi":"10.1093/ehjdh/ztae099","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Digital health is becoming increasingly powerful and available but is frequently not effectively integrated into daily practice. A hybrid programme was developed to provide holistic diagnostic and therapeutic patient care in atrial fibrillation.</p><p><strong>Methods and results: </strong>Patients (<i>n</i> = 68) were recruited at the electrophysiology centre following successful interventional restoration of sinus rhythm. The 12-month programme consists of the key modalities: (i) self-recording of one-lead electrocardiograms (ECGs), (ii) short-term remote ECG diagnosis and medical advice by video consultation, and (iii) App-based education on lifestyle and risk factor optimization with video consultation. Patients recorded 29 092 ECGs, averaging 1.42 ECGs/day. Recurrent arrhythmia was found and confirmed in 39 patients. In all cases, arrhythmia was first diagnosed based on wearable ECG over the platform, rather than by standard in-office ECG/Holter. No false positive occurred. Patients with recurred arrhythmia were treated by pulmonary vein isolation (<i>n</i> = 17), electric cardioversion (<i>n</i> = 17), antiarrhythmic medication (<i>n</i> = 5), or other interventional procedures (<i>n</i> = 1). Most patients (<i>n</i> = 30) scheduled a video consultation over the App as the first medical touchpoint after arrhythmia occurrence. In 21 patients with arterial hypertension, systolic blood pressure was reduced by 8.0 ± 8.6 mmHg (mean ± SD), <i>P</i> < 0.01. In 25 patients with obesity (body mass index ≥ 30), body weight was reduced by 3.6 ± 5.5 kg (mean ± SD), <i>P</i> < 0.01.</p><p><strong>Conclusion: </strong>This real-world analysis indicates that the hybrid holistic programme is applicable in daily practice and is actively followed by patients and improves diagnostic and therapeutic outcomes. These promising data need to be confirmed in a controlled randomized study.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"6 2","pages":"261-269"},"PeriodicalIF":4.4000,"publicationDate":"2025-01-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11914723/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztae099","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
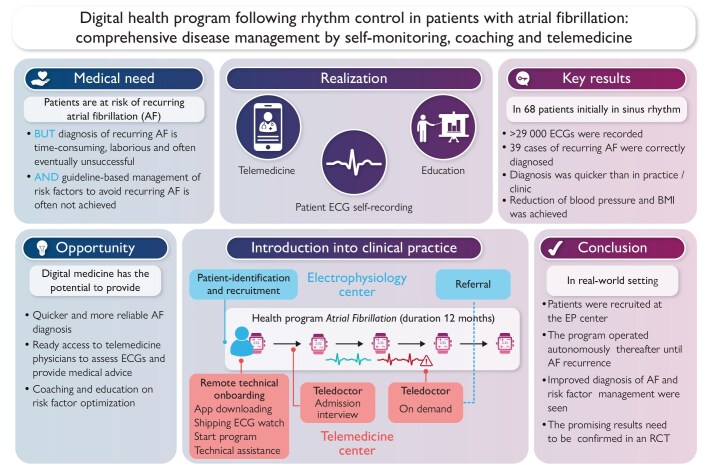
Aims: Digital health is becoming increasingly powerful and available but is frequently not effectively integrated into daily practice. A hybrid programme was developed to provide holistic diagnostic and therapeutic patient care in atrial fibrillation.
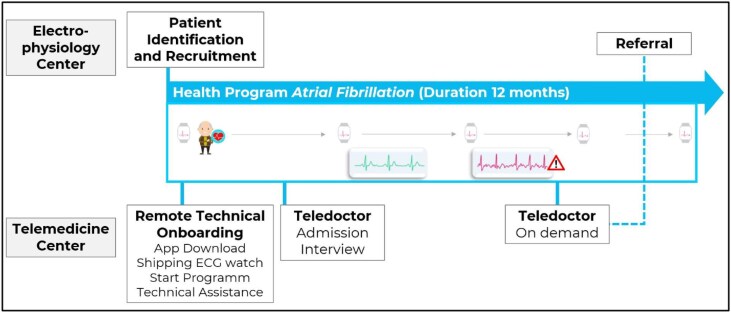
Methods and results: Patients (n = 68) were recruited at the electrophysiology centre following successful interventional restoration of sinus rhythm. The 12-month programme consists of the key modalities: (i) self-recording of one-lead electrocardiograms (ECGs), (ii) short-term remote ECG diagnosis and medical advice by video consultation, and (iii) App-based education on lifestyle and risk factor optimization with video consultation. Patients recorded 29 092 ECGs, averaging 1.42 ECGs/day. Recurrent arrhythmia was found and confirmed in 39 patients. In all cases, arrhythmia was first diagnosed based on wearable ECG over the platform, rather than by standard in-office ECG/Holter. No false positive occurred. Patients with recurred arrhythmia were treated by pulmonary vein isolation (n = 17), electric cardioversion (n = 17), antiarrhythmic medication (n = 5), or other interventional procedures (n = 1). Most patients (n = 30) scheduled a video consultation over the App as the first medical touchpoint after arrhythmia occurrence. In 21 patients with arterial hypertension, systolic blood pressure was reduced by 8.0 ± 8.6 mmHg (mean ± SD), P < 0.01. In 25 patients with obesity (body mass index ≥ 30), body weight was reduced by 3.6 ± 5.5 kg (mean ± SD), P < 0.01.
Conclusion: This real-world analysis indicates that the hybrid holistic programme is applicable in daily practice and is actively followed by patients and improves diagnostic and therapeutic outcomes. These promising data need to be confirmed in a controlled randomized study.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


