{"title":"Comparison of machine learning and conventional criteria in detecting left ventricular hypertrophy and prognosis with electrocardiography.","authors":"Jui-Tzu Huang, Chih-Hsueh Tseng, Wei-Ming Huang, Wen-Chung Yu, Hao-Min Cheng, Hsi-Lu Chao, Chern-En Chiang, Chen-Huan Chen, Albert C Yang, Shih-Hsien Sung","doi":"10.1093/ehjdh/ztaf003","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Left ventricular hypertrophy (LVH) is clinically important; current electrocardiography (ECG) diagnostic criteria are inadequate for early detection. This study aimed to develop an artificial intelligence (AI)-based algorithm to improve the accuracy and prognostic value of ECG criteria for LVH detection.</p><p><strong>Methods and results: </strong>A total of 42 016 patients (64.3 ± 16.5 years, 55.3% male) were enrolled. LV mass index was calculated from echocardiographic measurements. Left ventricular hypertrophy screening utilized ECG criteria, including Sokolow-Lyon, Cornell product, Cornell/strain index, Framingham criterion, and Peguero-Lo Presti. An AI algorithm using CatBoost was developed and validated (training dataset 80% and testing dataset 20%). F1 scores, reflecting the harmonic mean of precision and recall, were calculated. Mortality data were obtained through linkage with the National Death Registry. The CatBoost-based AI algorithm outperformed conventional ECG criteria in detecting LVH, achieving superior sensitivity, specificity, positive predictive value, F1 score, and area under curve. Significant features to predict LVH involved QRS and P-wave morphology. During a median follow-up duration of 10.1 years, 1655 deaths occurred in the testing dataset. Cox regression analyses showed that LVH identified by AI algorithm (hazard ratio and 95% confidence interval: 1.587, 1.309-1.924), Sokolow-Lyon (1.19, 1.038-1.365), Cornell product (1.301, 1.124-1.505), Cornell/strain index (1.306, 1.185-1.439), Framingham criterion (1.174, 1.062-1.298), and echocardiography-confirmed LVH (1.124, 1.019-1.239) were all significantly associated with mortality. Notably, AI-diagnosed LVH was more predictive of mortality than echocardiography-confirmed LVH.</p><p><strong>Conclusion: </strong>Artificial intelligence-based LVH diagnosis outperformed conventional ECG criteria and was a superior predictor of mortality compared to echocardiography-confirmed LVH.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"6 2","pages":"252-260"},"PeriodicalIF":4.4000,"publicationDate":"2025-02-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11914727/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztaf003","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Left ventricular hypertrophy (LVH) is clinically important; current electrocardiography (ECG) diagnostic criteria are inadequate for early detection. This study aimed to develop an artificial intelligence (AI)-based algorithm to improve the accuracy and prognostic value of ECG criteria for LVH detection.
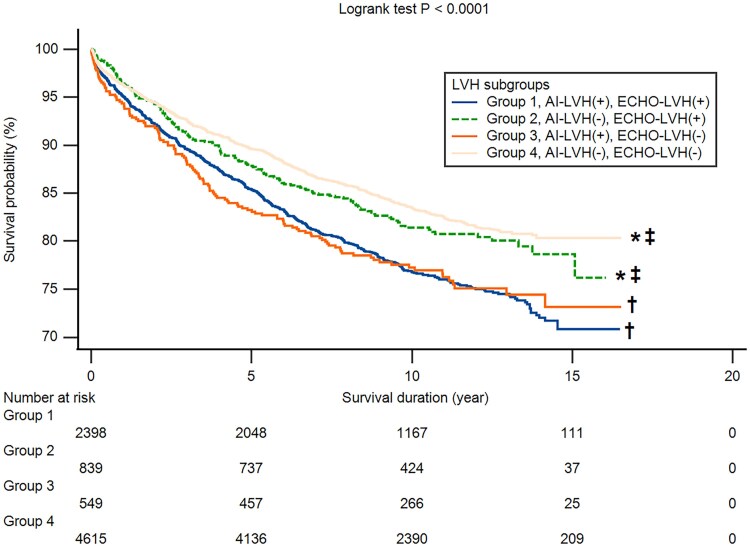
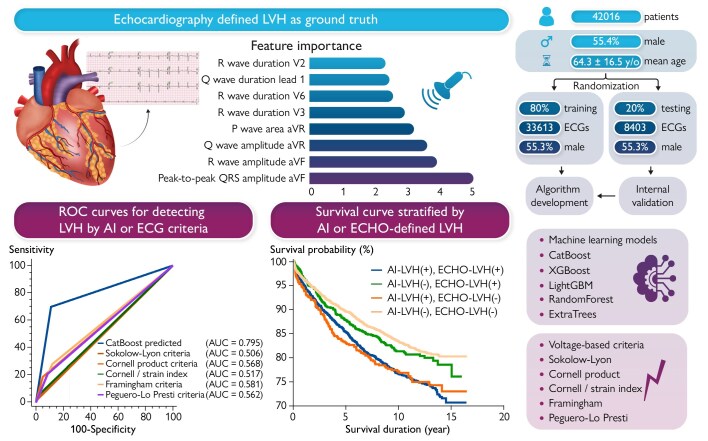
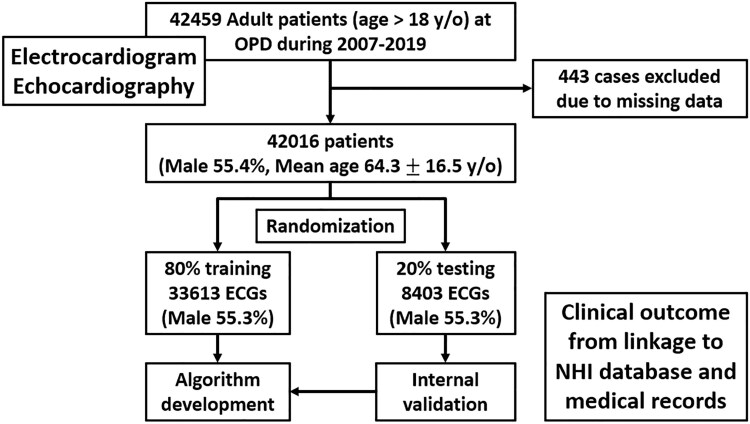
Methods and results: A total of 42 016 patients (64.3 ± 16.5 years, 55.3% male) were enrolled. LV mass index was calculated from echocardiographic measurements. Left ventricular hypertrophy screening utilized ECG criteria, including Sokolow-Lyon, Cornell product, Cornell/strain index, Framingham criterion, and Peguero-Lo Presti. An AI algorithm using CatBoost was developed and validated (training dataset 80% and testing dataset 20%). F1 scores, reflecting the harmonic mean of precision and recall, were calculated. Mortality data were obtained through linkage with the National Death Registry. The CatBoost-based AI algorithm outperformed conventional ECG criteria in detecting LVH, achieving superior sensitivity, specificity, positive predictive value, F1 score, and area under curve. Significant features to predict LVH involved QRS and P-wave morphology. During a median follow-up duration of 10.1 years, 1655 deaths occurred in the testing dataset. Cox regression analyses showed that LVH identified by AI algorithm (hazard ratio and 95% confidence interval: 1.587, 1.309-1.924), Sokolow-Lyon (1.19, 1.038-1.365), Cornell product (1.301, 1.124-1.505), Cornell/strain index (1.306, 1.185-1.439), Framingham criterion (1.174, 1.062-1.298), and echocardiography-confirmed LVH (1.124, 1.019-1.239) were all significantly associated with mortality. Notably, AI-diagnosed LVH was more predictive of mortality than echocardiography-confirmed LVH.
Conclusion: Artificial intelligence-based LVH diagnosis outperformed conventional ECG criteria and was a superior predictor of mortality compared to echocardiography-confirmed LVH.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


