Anton N Isaacs, Caroline Le Brun, Vaidy Swaminathan
{"title":"The design and implementation of an innovative indicated suicide prevention service in Melbourne.","authors":"Anton N Isaacs, Caroline Le Brun, Vaidy Swaminathan","doi":"10.1186/s40621-025-00567-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Suicide prevention strategies are targeted at three levels: the general population (Universal), persons at risk (Selected), and persons who have attempted suicide or have suicidal ideation (Indicated). This study describes the implementation of an innovative indicated suicide prevention service that prioritizes peer and psychosocial support at one of Australia's largest mental health services. The purpose of this paper is threefold. (1) To describe the process of designing and implementing an innovative indicated suicide prevention service in Melbourne (2) To compare the implementation framework developed around it with other relevant frameworks and (3) To describe its stages of care.</p><p><strong>Results: </strong>Based on the activities undertaken by the 'project champion' in designing and implementing Clayton HOPE, a pragmatic framework of implementation (PFI) was developed. The PFI included six steps. 1: Determine client needs; 2: Plan the model of care; 3: Determine the workforce and other resource requirements to achieve client needs; 4: Establish the workforce and finalize the team; 5: Facilitate stakeholder buy-in and 6: Regular monitoring and evaluation. The steps of the PFI, fit within the Quality Implementation Framework, albeit in a different sequence, owing to variations in settings, organizational circumstances, and readiness for change. The PFI also enhances the Levels of Change model by including additional requirements. A five-stage model of care was developed and implemented. They are 1: Early engagement and empathetic support (within 24 h of referral); 2: Assessment of psychosocial needs and suicidal risk (within 72 h of referral) 3: Construction of a personal safety plan (within 7 days of referral) 4: Implementation of the personal safety plan and risk management (week 2 - week12) and 5: Discharge and handover to ongoing supports (12 weeks from enrollment).</p><p><strong>Conclusions: </strong>The main implications of this work are twofold: (1) The implementation of innovative models of care can be achieved by a 'project champion' with the relevant experience, authority and determination when funding is available and (2) Indicated suicide prevention models of care can strike a balance between clinical and non-clinical interventions that are tailored to client needs.</p>","PeriodicalId":37379,"journal":{"name":"Injury Epidemiology","volume":"12 1","pages":"16"},"PeriodicalIF":2.2000,"publicationDate":"2025-03-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11921568/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Injury Epidemiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40621-025-00567-z","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Suicide prevention strategies are targeted at three levels: the general population (Universal), persons at risk (Selected), and persons who have attempted suicide or have suicidal ideation (Indicated). This study describes the implementation of an innovative indicated suicide prevention service that prioritizes peer and psychosocial support at one of Australia's largest mental health services. The purpose of this paper is threefold. (1) To describe the process of designing and implementing an innovative indicated suicide prevention service in Melbourne (2) To compare the implementation framework developed around it with other relevant frameworks and (3) To describe its stages of care.
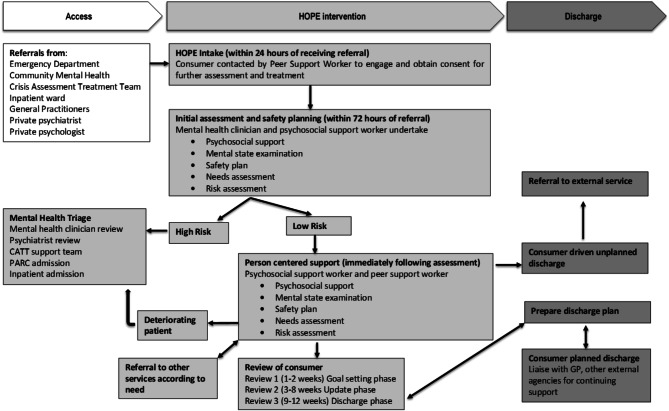
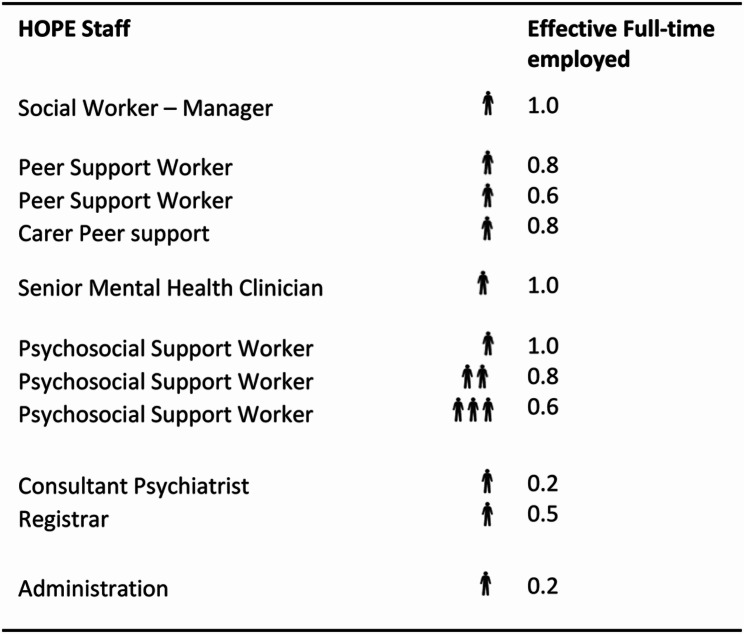
Results: Based on the activities undertaken by the 'project champion' in designing and implementing Clayton HOPE, a pragmatic framework of implementation (PFI) was developed. The PFI included six steps. 1: Determine client needs; 2: Plan the model of care; 3: Determine the workforce and other resource requirements to achieve client needs; 4: Establish the workforce and finalize the team; 5: Facilitate stakeholder buy-in and 6: Regular monitoring and evaluation. The steps of the PFI, fit within the Quality Implementation Framework, albeit in a different sequence, owing to variations in settings, organizational circumstances, and readiness for change. The PFI also enhances the Levels of Change model by including additional requirements. A five-stage model of care was developed and implemented. They are 1: Early engagement and empathetic support (within 24 h of referral); 2: Assessment of psychosocial needs and suicidal risk (within 72 h of referral) 3: Construction of a personal safety plan (within 7 days of referral) 4: Implementation of the personal safety plan and risk management (week 2 - week12) and 5: Discharge and handover to ongoing supports (12 weeks from enrollment).
Conclusions: The main implications of this work are twofold: (1) The implementation of innovative models of care can be achieved by a 'project champion' with the relevant experience, authority and determination when funding is available and (2) Indicated suicide prevention models of care can strike a balance between clinical and non-clinical interventions that are tailored to client needs.
期刊介绍:
Injury Epidemiology is dedicated to advancing the scientific foundation for injury prevention and control through timely publication and dissemination of peer-reviewed research. Injury Epidemiology aims to be the premier venue for communicating epidemiologic studies of unintentional and intentional injuries, including, but not limited to, morbidity and mortality from motor vehicle crashes, drug overdose/poisoning, falls, drowning, fires/burns, iatrogenic injury, suicide, homicide, assaults, and abuse. We welcome investigations designed to understand the magnitude, distribution, determinants, causes, prevention, diagnosis, treatment, prognosis, and outcomes of injuries in specific population groups, geographic regions, and environmental settings (e.g., home, workplace, transport, recreation, sports, and urban/rural). Injury Epidemiology has a special focus on studies generating objective and practical knowledge that can be translated into interventions to reduce injury morbidity and mortality on a population level. Priority consideration will be given to manuscripts that feature contemporary theories and concepts, innovative methods, and novel techniques as applied to injury surveillance, risk assessment, development and implementation of effective interventions, and program and policy evaluation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


