{"title":"New index for distinguishing between critical illness myopathy and neuromyopathy: CMAP amplitude/duration index.","authors":"Handan Uzunçakmak Uyanik, Fatma Gökçem Yildiz, Çağrı Mesut Temuçin","doi":"10.55730/1300-0144.5949","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/aim: </strong>Critical illness-associated weakness is a common neuromuscular syndrome that may manifest as critical illness myopathy (CIM), critical illness polyneuropathy (CIP), or an overlapping syndrome known as critical illness polyneuromyopathy (CIPM). Distinguishing between these subtypes can be challenging due to technical issues, patient-related factors such as insufficient cooperation with needle electromyography (EMG) or edema, and the need for sophisticated, time-consuming electrophysiological methods and invasive procedures such as biopsy. This study aimed to contribute to the electrophysiological distinction between CIM and CIPM.</p><p><strong>Materials and methods: </strong>A new index was designed based on distal compound muscle action potential (CMAP) amplitude and negative peak duration values. Comparative and receiver operating characteristic curve analyses were performed on the parameters of patients with CIM and CIPM, as well as between patient groups and controls.</p><p><strong>Results: </strong>The median and ulnar CMAP index cut-off values for distinguishing between CIM and CIPM were determined to be 0.35 and 0.51, respectively. Values below these cut-off points support a diagnosis of CIPM while higher values indicate CIM. The best parameter for distinguishing both CIM and CIPM patients from healthy controls was the peroneal CMAP index, with a cut-off value of 0.45.</p><p><strong>Conclusion: </strong>The CMAP index can be easily calculated from CMAP values obtained during routine nerve conduction studies. This index may serve as a practical and guiding method for differentiating between CIM and CIPM, contributing to the electrophysiological diagnosis of critically ill patients, and particularly those with unreliable sensory nerve action potentials and needle EMG examinations.</p>","PeriodicalId":23361,"journal":{"name":"Turkish Journal of Medical Sciences","volume":"55 1","pages":"112-120"},"PeriodicalIF":1.0000,"publicationDate":"2024-12-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11913521/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Turkish Journal of Medical Sciences","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.55730/1300-0144.5949","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background/aim: Critical illness-associated weakness is a common neuromuscular syndrome that may manifest as critical illness myopathy (CIM), critical illness polyneuropathy (CIP), or an overlapping syndrome known as critical illness polyneuromyopathy (CIPM). Distinguishing between these subtypes can be challenging due to technical issues, patient-related factors such as insufficient cooperation with needle electromyography (EMG) or edema, and the need for sophisticated, time-consuming electrophysiological methods and invasive procedures such as biopsy. This study aimed to contribute to the electrophysiological distinction between CIM and CIPM.
Materials and methods: A new index was designed based on distal compound muscle action potential (CMAP) amplitude and negative peak duration values. Comparative and receiver operating characteristic curve analyses were performed on the parameters of patients with CIM and CIPM, as well as between patient groups and controls.
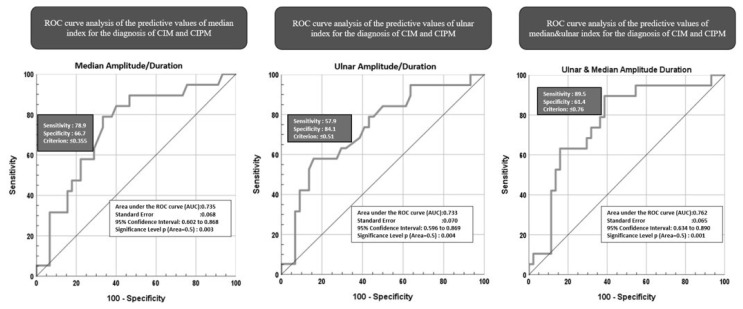
Results: The median and ulnar CMAP index cut-off values for distinguishing between CIM and CIPM were determined to be 0.35 and 0.51, respectively. Values below these cut-off points support a diagnosis of CIPM while higher values indicate CIM. The best parameter for distinguishing both CIM and CIPM patients from healthy controls was the peroneal CMAP index, with a cut-off value of 0.45.
Conclusion: The CMAP index can be easily calculated from CMAP values obtained during routine nerve conduction studies. This index may serve as a practical and guiding method for differentiating between CIM and CIPM, contributing to the electrophysiological diagnosis of critically ill patients, and particularly those with unreliable sensory nerve action potentials and needle EMG examinations.
期刊介绍:
Turkish Journal of Medical sciences is a peer-reviewed comprehensive resource that provides critical up-to-date information on the broad spectrum of general medical sciences. The Journal intended to publish original medical scientific papers regarding the priority based on the prominence, significance, and timeliness of the findings. However since the audience of the Journal is not limited to any subspeciality in a wide variety of medical disciplines, the papers focusing on the technical details of a given medical subspeciality may not be evaluated for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


