{"title":"Engineering the bone reconstruction surgery: the case of the masquelet-induced membrane technique.","authors":"Marjorie Durand, Laurent Mathieu, Julien Venant, Alain-Charles Masquelet, Jean-Marc Collombet","doi":"10.1007/s00068-025-02815-9","DOIUrl":null,"url":null,"abstract":"<p><p>The reconstruction of large bone defects remains challenging for orthopedic surgeons. Autologous bone grafts (ABGs) are the gold standard treatment for limited size defects, but larger bone defects (> 5 cm) require the use of more sophisticated techniques, such as the Masquelet technique. Over the last three decades, the Masquelet or induced membrane technique (IMT) has become increasingly popular as it does not require high-precision microsurgery skills and the time taken to achieve bone consolidation is independent of the length of the defect. IMT is a two-stage procedure. In the first stage, a polymethylmethacrylate (PMMA) cement spacer is implanted into the bone lesion and a physiological immune reaction initiates the formation of a fibrotic induced membrane (IM) with both angiogenic and osteogenic properties. The second stage, performed several weeks later, involves removal of the spacer followed by the implantation of a standard ABG in the preserved IM cavity for subsequent bone repair. In this extensive review, we explain how the success of this surgical procedure can be attributed to the synergy of four key components: the inducer (the PMMA cement), the recipient (the IM), the effector (the bone graft) and the modulator (the mechanical environment). Conversely, we then explain how each key component can contribute to the failure of such treatment. Finally, we discuss existing or emerging innovative and biotechnology-oriented strategies for optimizing surgical outcome with respect to the four components of IMT described above.</p>","PeriodicalId":12064,"journal":{"name":"European Journal of Trauma and Emergency Surgery","volume":"51 1","pages":"138"},"PeriodicalIF":2.2000,"publicationDate":"2025-03-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11919993/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Trauma and Emergency Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00068-025-02815-9","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
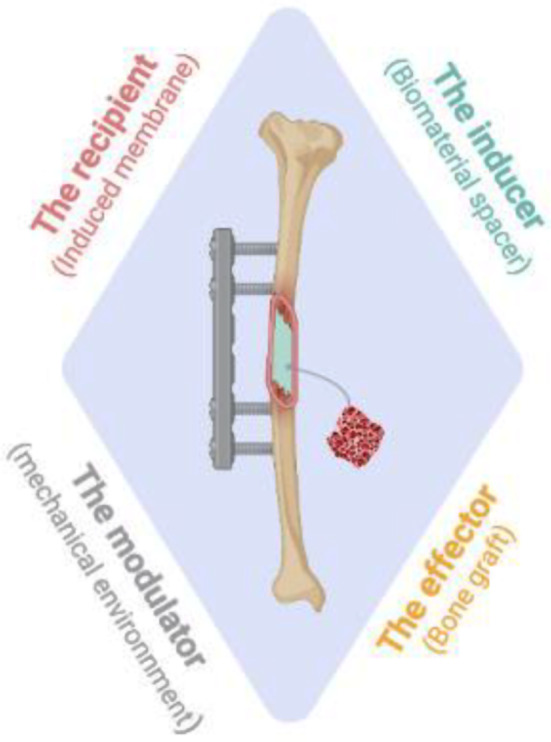
The reconstruction of large bone defects remains challenging for orthopedic surgeons. Autologous bone grafts (ABGs) are the gold standard treatment for limited size defects, but larger bone defects (> 5 cm) require the use of more sophisticated techniques, such as the Masquelet technique. Over the last three decades, the Masquelet or induced membrane technique (IMT) has become increasingly popular as it does not require high-precision microsurgery skills and the time taken to achieve bone consolidation is independent of the length of the defect. IMT is a two-stage procedure. In the first stage, a polymethylmethacrylate (PMMA) cement spacer is implanted into the bone lesion and a physiological immune reaction initiates the formation of a fibrotic induced membrane (IM) with both angiogenic and osteogenic properties. The second stage, performed several weeks later, involves removal of the spacer followed by the implantation of a standard ABG in the preserved IM cavity for subsequent bone repair. In this extensive review, we explain how the success of this surgical procedure can be attributed to the synergy of four key components: the inducer (the PMMA cement), the recipient (the IM), the effector (the bone graft) and the modulator (the mechanical environment). Conversely, we then explain how each key component can contribute to the failure of such treatment. Finally, we discuss existing or emerging innovative and biotechnology-oriented strategies for optimizing surgical outcome with respect to the four components of IMT described above.
期刊介绍:
The European Journal of Trauma and Emergency Surgery aims to open an interdisciplinary forum that allows for the scientific exchange between basic and clinical science related to pathophysiology, diagnostics and treatment of traumatized patients. The journal covers all aspects of clinical management, operative treatment and related research of traumatic injuries.
Clinical and experimental papers on issues relevant for the improvement of trauma care are published. Reviews, original articles, short communications and letters allow the appropriate presentation of major and minor topics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


