Jagoš Golubović, Petar Vuleković, Djula Djilvesi, Nenad Krajčinović, Igor Horvat, Bojan Jelača, Filip Pajičić, Nebojša Lasica, Srđan Stošić, Ante Rotim, Lukas Rasulić
{"title":"COMPUTED TOMOGRAPHY SCORING SCALES AS EARLY OUTCOME PREDICTORS IN PATIENTS WITH TRAUMATIC BRAIN INJURY: WHICH ONE TO USE?","authors":"Jagoš Golubović, Petar Vuleković, Djula Djilvesi, Nenad Krajčinović, Igor Horvat, Bojan Jelača, Filip Pajičić, Nebojša Lasica, Srđan Stošić, Ante Rotim, Lukas Rasulić","doi":"10.20471/acc.2024.63.02.11","DOIUrl":null,"url":null,"abstract":"<p><p>Computed tomography (CT) is an essential tool in diagnosing and treating traumatic brain injury (TBI). Marshall CT classification, Rotterdam and Helsinki CT scores were consecutively developed as prediction outcome scales by computing TBI CT abnormalities. None of them classifies the pathological CT findings in the same manner. We aimed to determine which one is most accurate and has the best grading discriminatory power in determining early outcome. All TBI patients treated at a single center in a one-year period having undergone a CT scan on admission were retrospectively included. After calculation of all three scores, comparison among scale performances, as well as their accuracy in predicting patient 6-month outcome by the Glasgow Outcome Scale (GOS) was made. We used the Receiver Operating Characteristic curves to analyze correlation between all scales and early outcome. We calculated the area under the curve (AUC) to determine the power of each system while paired samples T-test was used to determine correlation among the scales. Mann-Whitney U test was performed to determine difference in outcome groups. A total of 1006 patients were included in final analysis. The mean patient age at presentation was 55.6 (±20.1) years, overall mortality was 6.4%, mean GOS was 3.00 (±1.4), and mean Glasgow Coma Score (GCS) was 13.9 (±0.2). Mortality was higher among patients with lower scores (p<0.01 all). The AUCs indicated that all scoring systems had a similarly high discriminative power in predicting early unfavorable outcome (Marshall AUC 0.86 <i>vs</i>. Rotterdam AUC 0.82 <i>vs</i>. Helsinki AUC 0.84). High correlation was found between Marshall and Rotterdam grading, r = 0.78, and moderate correlation between the other two pairs (Marshall <i>vs</i>. Helsinki, r=0.62, and Rotterdam <i>vs</i>. Helsinki, r=0.51). Additionally, low GCS and high injury severity score (ISS) could be identified as strong predictors of early death and poor outcome. In conclusion, all classification systems demonstrated a similar, strong predictive power for early outcome, but even greater discrimination results could be obtained if GCS and ISS were incorporated in the calculation. Helsinki CT score was least predictable of all three, and had the lowest correlation with the other two. Although Marshall CT classification was the oldest and simplest, it had at least the same prediction power as the newer scoring scales and should remain in use. Therefore, for prognostic purposes, this study recommends using one individual scale in clinical application to get the best possible prediction for TBI.</p>","PeriodicalId":7072,"journal":{"name":"Acta clinica Croatica","volume":"63 2","pages":"351-357"},"PeriodicalIF":0.8000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11912857/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta clinica Croatica","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.20471/acc.2024.63.02.11","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
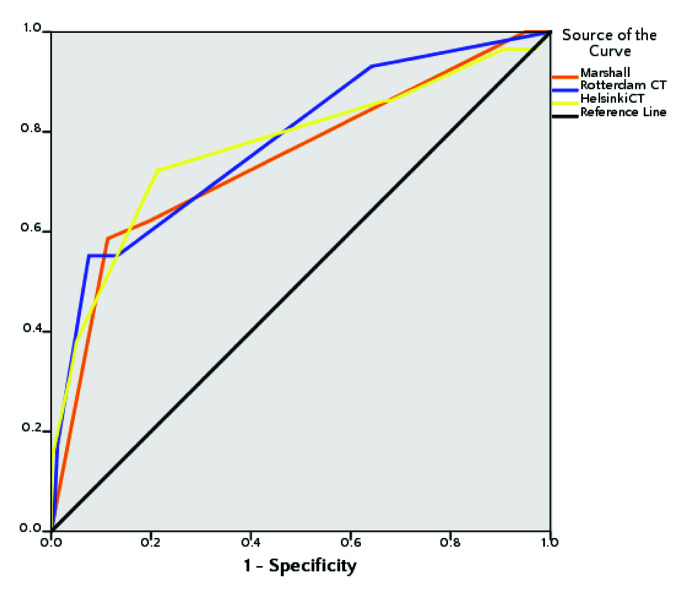
Computed tomography (CT) is an essential tool in diagnosing and treating traumatic brain injury (TBI). Marshall CT classification, Rotterdam and Helsinki CT scores were consecutively developed as prediction outcome scales by computing TBI CT abnormalities. None of them classifies the pathological CT findings in the same manner. We aimed to determine which one is most accurate and has the best grading discriminatory power in determining early outcome. All TBI patients treated at a single center in a one-year period having undergone a CT scan on admission were retrospectively included. After calculation of all three scores, comparison among scale performances, as well as their accuracy in predicting patient 6-month outcome by the Glasgow Outcome Scale (GOS) was made. We used the Receiver Operating Characteristic curves to analyze correlation between all scales and early outcome. We calculated the area under the curve (AUC) to determine the power of each system while paired samples T-test was used to determine correlation among the scales. Mann-Whitney U test was performed to determine difference in outcome groups. A total of 1006 patients were included in final analysis. The mean patient age at presentation was 55.6 (±20.1) years, overall mortality was 6.4%, mean GOS was 3.00 (±1.4), and mean Glasgow Coma Score (GCS) was 13.9 (±0.2). Mortality was higher among patients with lower scores (p<0.01 all). The AUCs indicated that all scoring systems had a similarly high discriminative power in predicting early unfavorable outcome (Marshall AUC 0.86 vs. Rotterdam AUC 0.82 vs. Helsinki AUC 0.84). High correlation was found between Marshall and Rotterdam grading, r = 0.78, and moderate correlation between the other two pairs (Marshall vs. Helsinki, r=0.62, and Rotterdam vs. Helsinki, r=0.51). Additionally, low GCS and high injury severity score (ISS) could be identified as strong predictors of early death and poor outcome. In conclusion, all classification systems demonstrated a similar, strong predictive power for early outcome, but even greater discrimination results could be obtained if GCS and ISS were incorporated in the calculation. Helsinki CT score was least predictable of all three, and had the lowest correlation with the other two. Although Marshall CT classification was the oldest and simplest, it had at least the same prediction power as the newer scoring scales and should remain in use. Therefore, for prognostic purposes, this study recommends using one individual scale in clinical application to get the best possible prediction for TBI.
期刊介绍:
Acta Clinica Croatica is a peer reviewed general medical journal that publishes original articles that advance and improve medical science and practice and that serve the purpose of transfer of original and valuable information to journal readers. Acta Clinica Croatica is published in English four times a year.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


