Y Hamada, R Mukora, R Pelusa, T Ntshiqa, J Shedrawy, K Velen, I Abubakar, S Charalambous, S Walker, M X Rangaka
{"title":"Costs and cost-effectiveness of integrated screening for non-communicable diseases in TB contacts.","authors":"Y Hamada, R Mukora, R Pelusa, T Ntshiqa, J Shedrawy, K Velen, I Abubakar, S Charalambous, S Walker, M X Rangaka","doi":"10.5588/ijtldopen.24.0625","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Integrating non-communicable disease (NCD) screening into TB household contact investigations may identify undiagnosed NCDs and reduce the burden of both conditions. However, evidence on the costs and cost-effectiveness of this approach is limited.</p><p><strong>Method: </strong>We conducted a cross-sectional study in South Africa to assess patient and provider costs for NCD screening (hypertension, diabetes, chronic kidney disease, dyslipidaemia). Incremental costs per NCD case identified were calculated. Using a decision tree model, we estimated incremental costs per disability-adjusted life year (DALY) averted over 10 years from a healthcare perspective, with cardiovascular disease (CVD) risk estimated using the WHO prediction model.</p><p><strong>Results: </strong>The incremental cost was USD72.3 per contact screened and USD334.0 per NCD case identified. Integrated screening reduced mean 10-year CVD risk from 5.7% to 2.7% among contacts with NCDs. The incremental cost-effectiveness ratio (ICER) was USD27,043.6 per DALY averted, exceeding South Africa's threshold of USD3,708. Management of identified NCDs, mainly drug costs, comprised over 80% of total incremental costs. The ICER decreased in populations with a high risk for NCDs.</p><p><strong>Conclusion: </strong>Integrated NCD screening was not cost-effective, mainly due to subsequent care costs. Prioritising individuals at high risk for NCDs can improve cost-effectiveness.</p>","PeriodicalId":519984,"journal":{"name":"IJTLD open","volume":"2 3","pages":"160-165"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11906026/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"IJTLD open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5588/ijtldopen.24.0625","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Integrating non-communicable disease (NCD) screening into TB household contact investigations may identify undiagnosed NCDs and reduce the burden of both conditions. However, evidence on the costs and cost-effectiveness of this approach is limited.
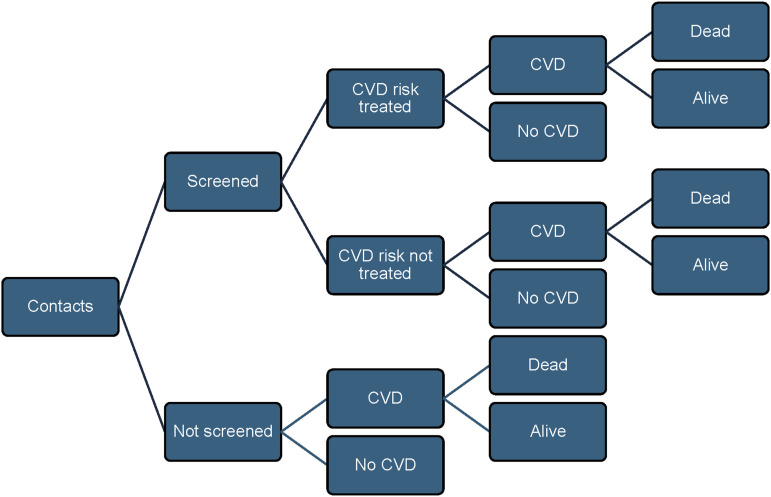
Method: We conducted a cross-sectional study in South Africa to assess patient and provider costs for NCD screening (hypertension, diabetes, chronic kidney disease, dyslipidaemia). Incremental costs per NCD case identified were calculated. Using a decision tree model, we estimated incremental costs per disability-adjusted life year (DALY) averted over 10 years from a healthcare perspective, with cardiovascular disease (CVD) risk estimated using the WHO prediction model.
Results: The incremental cost was USD72.3 per contact screened and USD334.0 per NCD case identified. Integrated screening reduced mean 10-year CVD risk from 5.7% to 2.7% among contacts with NCDs. The incremental cost-effectiveness ratio (ICER) was USD27,043.6 per DALY averted, exceeding South Africa's threshold of USD3,708. Management of identified NCDs, mainly drug costs, comprised over 80% of total incremental costs. The ICER decreased in populations with a high risk for NCDs.
Conclusion: Integrated NCD screening was not cost-effective, mainly due to subsequent care costs. Prioritising individuals at high risk for NCDs can improve cost-effectiveness.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


