{"title":"U shaped relationship between mean arterial pressure and 28 day mortality in ICU patients with acute myocardial infarction.","authors":"Qing Cui, Ping Jin, Yifan Ren, Pei Yang, Xiaoan Chen, Cheng Lian","doi":"10.1038/s41598-025-92648-8","DOIUrl":null,"url":null,"abstract":"<p><p>The current study aims to investigate the correlation between mean arterial pressure (MAP) and the risk of 28-day mortality in patients with acute myocardial infarction. This is a retrospective cohort study utilizing data from the eICU database, focusing on patients with acute myocardial infarction. We employed a multivariable logistic regression model to estimate the relationship between MAP and the 28-day mortality rate. Among 8161 patients with a median age of 67 years, 602 (7.38%) died within 28 days of ICU admission. Smooth curve fitting and generalized additive model analysis identified a threshold effect at MAP of 84 mmHg. We found that when MAP is less than 84 mmHg, a 10 mmHg increase in MAP reduces the mortality rate by approximately 40.13%. Specifically, for every 1 mmHg increase in MAP within this range, the mortality rate decreases significantly by 5% (OR = 0.95, 95% CI (0.93, 0.96), p < 0.0001). Conversely, above the threshold (MAP ≥ 84 mmHg), for every 10 mmHg increase, the mortality rate increases by 34.39% (OR = 1.3439, calculated based on the fact that a 1 mmHg MAP increase causes a 3% mortality rise (OR = 1.03, 95% CI (1.02, 1.03), p < 0.0001), showing a U-shaped association between MAP and 28-day mortality. We found that the baseline MAP at ICU admission, when in the range of 57-110 mmHg, was associated with the lowest 28-day all-cause mortality risk. The relationship between MAP and the risk of 28-day mortality forms a U-shaped curve, indicating that both higher and lower MAP levels are associated with an increased risk of 28-day mortality in ICU-admitted patients.</p>","PeriodicalId":21811,"journal":{"name":"Scientific Reports","volume":"15 1","pages":"9064"},"PeriodicalIF":3.9000,"publicationDate":"2025-03-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11914078/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scientific Reports","FirstCategoryId":"103","ListUrlMain":"https://doi.org/10.1038/s41598-025-92648-8","RegionNum":2,"RegionCategory":"综合性期刊","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MULTIDISCIPLINARY SCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
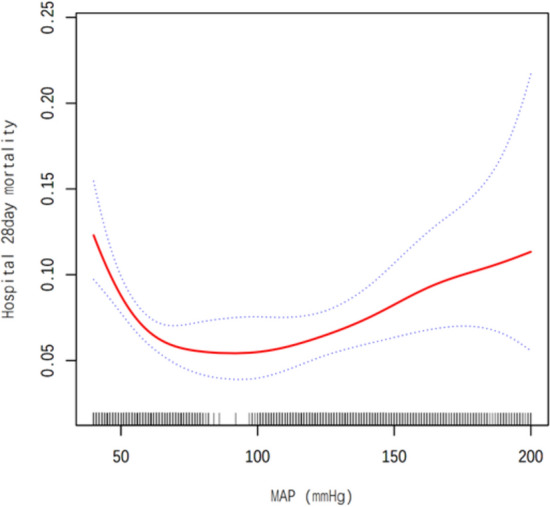
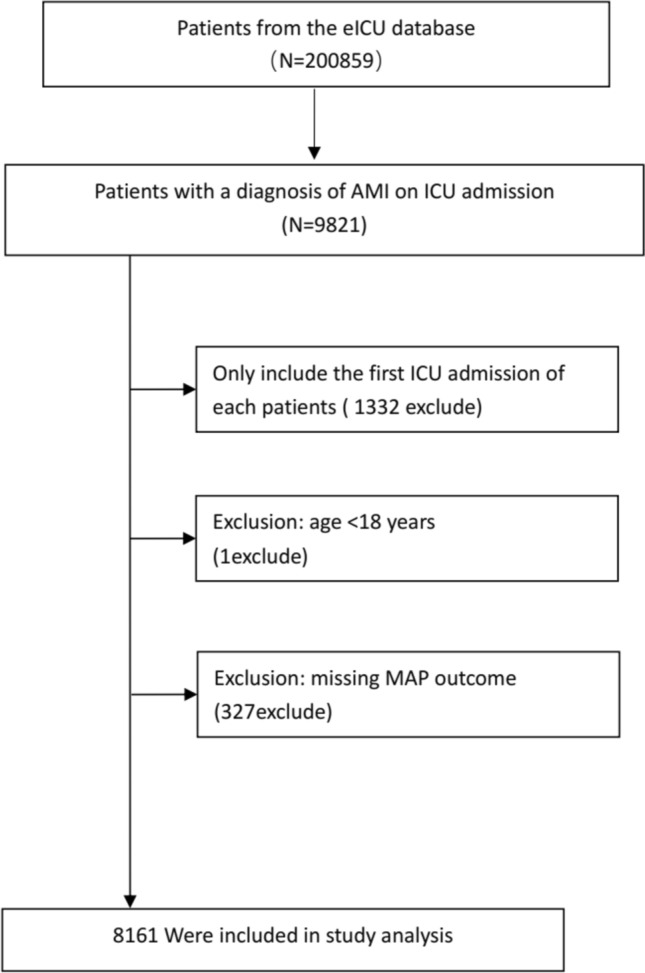
The current study aims to investigate the correlation between mean arterial pressure (MAP) and the risk of 28-day mortality in patients with acute myocardial infarction. This is a retrospective cohort study utilizing data from the eICU database, focusing on patients with acute myocardial infarction. We employed a multivariable logistic regression model to estimate the relationship between MAP and the 28-day mortality rate. Among 8161 patients with a median age of 67 years, 602 (7.38%) died within 28 days of ICU admission. Smooth curve fitting and generalized additive model analysis identified a threshold effect at MAP of 84 mmHg. We found that when MAP is less than 84 mmHg, a 10 mmHg increase in MAP reduces the mortality rate by approximately 40.13%. Specifically, for every 1 mmHg increase in MAP within this range, the mortality rate decreases significantly by 5% (OR = 0.95, 95% CI (0.93, 0.96), p < 0.0001). Conversely, above the threshold (MAP ≥ 84 mmHg), for every 10 mmHg increase, the mortality rate increases by 34.39% (OR = 1.3439, calculated based on the fact that a 1 mmHg MAP increase causes a 3% mortality rise (OR = 1.03, 95% CI (1.02, 1.03), p < 0.0001), showing a U-shaped association between MAP and 28-day mortality. We found that the baseline MAP at ICU admission, when in the range of 57-110 mmHg, was associated with the lowest 28-day all-cause mortality risk. The relationship between MAP and the risk of 28-day mortality forms a U-shaped curve, indicating that both higher and lower MAP levels are associated with an increased risk of 28-day mortality in ICU-admitted patients.
期刊介绍:
We publish original research from all areas of the natural sciences, psychology, medicine and engineering. You can learn more about what we publish by browsing our specific scientific subject areas below or explore Scientific Reports by browsing all articles and collections.
Scientific Reports has a 2-year impact factor: 4.380 (2021), and is the 6th most-cited journal in the world, with more than 540,000 citations in 2020 (Clarivate Analytics, 2021).
•Engineering
Engineering covers all aspects of engineering, technology, and applied science. It plays a crucial role in the development of technologies to address some of the world''s biggest challenges, helping to save lives and improve the way we live.
•Physical sciences
Physical sciences are those academic disciplines that aim to uncover the underlying laws of nature — often written in the language of mathematics. It is a collective term for areas of study including astronomy, chemistry, materials science and physics.
•Earth and environmental sciences
Earth and environmental sciences cover all aspects of Earth and planetary science and broadly encompass solid Earth processes, surface and atmospheric dynamics, Earth system history, climate and climate change, marine and freshwater systems, and ecology. It also considers the interactions between humans and these systems.
•Biological sciences
Biological sciences encompass all the divisions of natural sciences examining various aspects of vital processes. The concept includes anatomy, physiology, cell biology, biochemistry and biophysics, and covers all organisms from microorganisms, animals to plants.
•Health sciences
The health sciences study health, disease and healthcare. This field of study aims to develop knowledge, interventions and technology for use in healthcare to improve the treatment of patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


