Is chitosan-based dressing more effective than gauze pressure in achieving early hemostasis after dental extractions in patients with deranged coagulation profiles?
{"title":"Is chitosan-based dressing more effective than gauze pressure in achieving early hemostasis after dental extractions in patients with deranged coagulation profiles?","authors":"Satnam Singh Jolly, Vidya Rattan","doi":"10.7181/acfs.2024.0082","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Chitosan, a cationic polysaccharide, exerts hemostatic activity by promoting platelet adhesion and aggregation. This clinical study aimed to evaluate the effectiveness of chitosan-based dental dressing in achieving early local hemostasis, in comparison to gauze packs, after dental extractions in patients with deranged coagulation profiles.</p><p><strong>Methods: </strong>This study included 102 patients (204 extraction sites), of whom 86 were on anticoagulant therapy,15 had liver cirrhosis, and one with thrombocytopenic purpura required two or more tooth extractions. These sites were randomly divided into test and control sites. Patients with deranged coagulation profiles, including an international normalized ratio of 1.5-4, altered prothrombin time, activated partial thromboplastin time, and decreased platelet counts, were selected. Hemostasis was assessed at 10, 30, and 60 minutes post-extraction. Patients were evaluated on days 1, 3, and 7 for dry sockets and other adverse effects.</p><p><strong>Results: </strong>Hemostasis was achieved in 83.1% of test sites within 10 minutes, compared to only 18.8% of control sites. By 30 minutes, an additional 16.8% of test sites had achieved hemostasis versus an additional 16.7% of control sites. By 60 minutes, a further 5.9% of test sites had achieved hemostasis, compared to 63.7% of control sites. The mean postoperative hemostasis times were 15.10± 12.88 minutes for test sites and 45.20± 20.62 minutes for control sites. Dry socket incidence was slightly higher in test sites, but this tendency was not statistically significant (p>0.05).</p><p><strong>Conclusion: </strong>The study suggests that chitosan-based dental dressing facilitates early local hemostasis after tooth extraction in anticoagulated patients or patients with bleeding disorders.</p>","PeriodicalId":52238,"journal":{"name":"Archives of Craniofacial Surgery","volume":" ","pages":"65-69"},"PeriodicalIF":0.0000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12061772/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of Craniofacial Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7181/acfs.2024.0082","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/14 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Chitosan, a cationic polysaccharide, exerts hemostatic activity by promoting platelet adhesion and aggregation. This clinical study aimed to evaluate the effectiveness of chitosan-based dental dressing in achieving early local hemostasis, in comparison to gauze packs, after dental extractions in patients with deranged coagulation profiles.
Methods: This study included 102 patients (204 extraction sites), of whom 86 were on anticoagulant therapy,15 had liver cirrhosis, and one with thrombocytopenic purpura required two or more tooth extractions. These sites were randomly divided into test and control sites. Patients with deranged coagulation profiles, including an international normalized ratio of 1.5-4, altered prothrombin time, activated partial thromboplastin time, and decreased platelet counts, were selected. Hemostasis was assessed at 10, 30, and 60 minutes post-extraction. Patients were evaluated on days 1, 3, and 7 for dry sockets and other adverse effects.
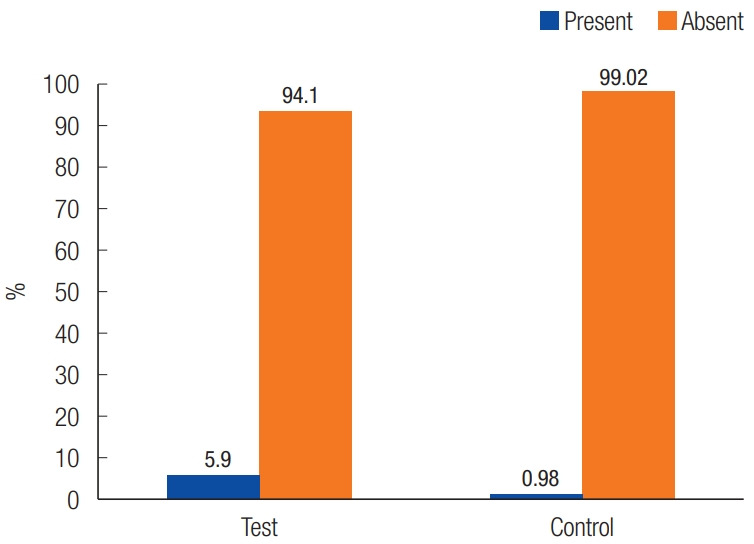
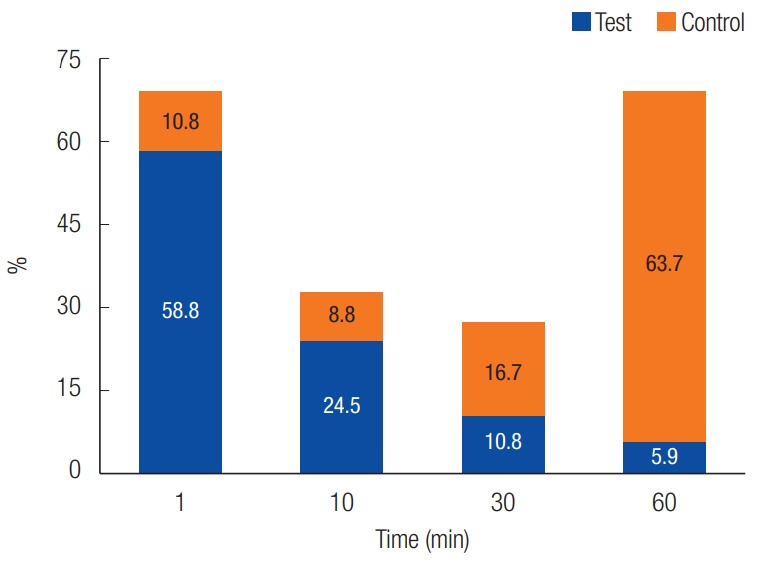
Results: Hemostasis was achieved in 83.1% of test sites within 10 minutes, compared to only 18.8% of control sites. By 30 minutes, an additional 16.8% of test sites had achieved hemostasis versus an additional 16.7% of control sites. By 60 minutes, a further 5.9% of test sites had achieved hemostasis, compared to 63.7% of control sites. The mean postoperative hemostasis times were 15.10± 12.88 minutes for test sites and 45.20± 20.62 minutes for control sites. Dry socket incidence was slightly higher in test sites, but this tendency was not statistically significant (p>0.05).
Conclusion: The study suggests that chitosan-based dental dressing facilitates early local hemostasis after tooth extraction in anticoagulated patients or patients with bleeding disorders.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


