Smoking and Elevated Preneoadjuvant Chemoradiotherapy Serum Carcinoembryonic Antigen Levels Are Associated With High Tumor Regression Grade and Poor Survival in Patients With Locally Advanced Rectal Cancer.
Jen-Pin Chuang, Hsiang-Lin Tsai, Po-Jung Chen, Ching-Wen Huang, Wei-Chih Su, Tsung-Kun Chang, Yen-Cheng Chen, Ching-Chun Li, Yung-Sung Yeh, Jaw-Yuan Wang
{"title":"Smoking and Elevated Preneoadjuvant Chemoradiotherapy Serum Carcinoembryonic Antigen Levels Are Associated With High Tumor Regression Grade and Poor Survival in Patients With Locally Advanced Rectal Cancer.","authors":"Jen-Pin Chuang, Hsiang-Lin Tsai, Po-Jung Chen, Ching-Wen Huang, Wei-Chih Su, Tsung-Kun Chang, Yen-Cheng Chen, Ching-Chun Li, Yung-Sung Yeh, Jaw-Yuan Wang","doi":"10.1002/kjm2.70008","DOIUrl":null,"url":null,"abstract":"<p><p>Neoadjuvant chemoradiotherapy (NACRT) is the standard treatment for patients with locally advanced rectal cancer (LARC). Tumor regression grade (TRG) is an essential prognostic factor in determining treatment efficacy. However, the potential factors influencing TRG in patients with rectal cancer who have received NACRT have not been investigated. We conducted a retrospective analysis of patients with LARC who received NACRT followed by surgical resection. We collected data on the patient characteristics, including age, sex, comorbidities, tumor size, lymph node status, time between NACRT and surgery, and pretreatment carcinoembryonic antigen (CEA) levels. TRG was determined on the basis of a pathological assessment of resected specimens, and overall survival (OS) at 5 years was determined. Univariate and multivariate logistic regression models were employed to evaluate the association between the patient characteristics and TRG. Univariate analysis revealed that smoking and prechemoradiotherapy (pre-CRT) and preoperative CEA levels were significantly associated with TRG. In a multivariate analysis, both smoking and higher pre-CRT CEA levels were identified as significant predictors of a high TRG. The hazard ratios were 2.32 (95% confidence interval [CI]: 1.06-5.07, p = 0.036) for smoking and 3.1 (95% CI: 1.69-5.68, p < 0.001) for higher pre-CRT CEA levels. In Kaplan-Meier analysis, the nonsmoker group exhibited higher OS (p = 0.004). Elevated pre-CRT CEA levels and current smoking status were associated with a more than two fold increase in the risk of a higher TRG after NACRT. Moreover, smoking was a significant risk factor for poor OS in patients with LARC following NACRT.</p>","PeriodicalId":94244,"journal":{"name":"The Kaohsiung journal of medical sciences","volume":" ","pages":"e70008"},"PeriodicalIF":3.1000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12199573/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Kaohsiung journal of medical sciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/kjm2.70008","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/13 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
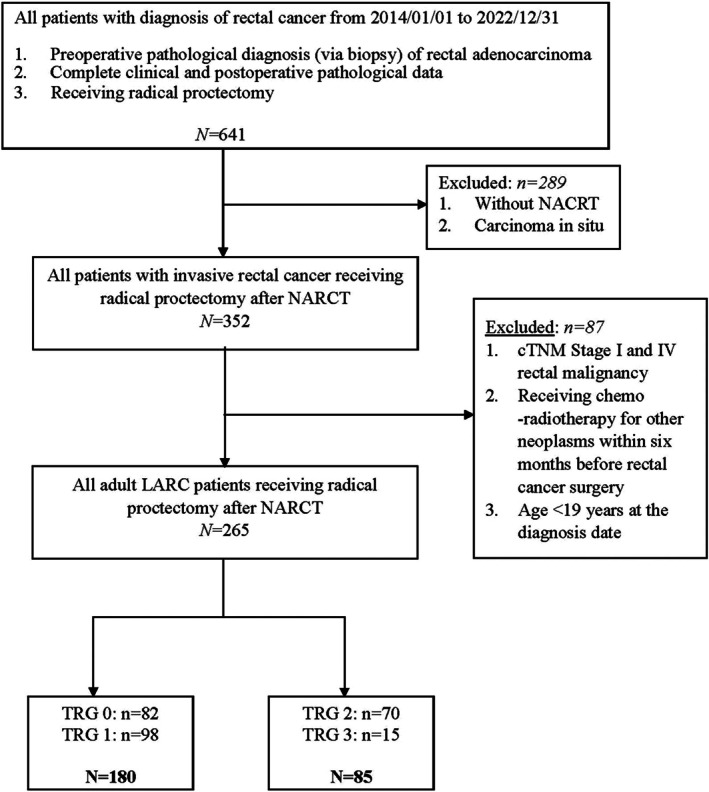
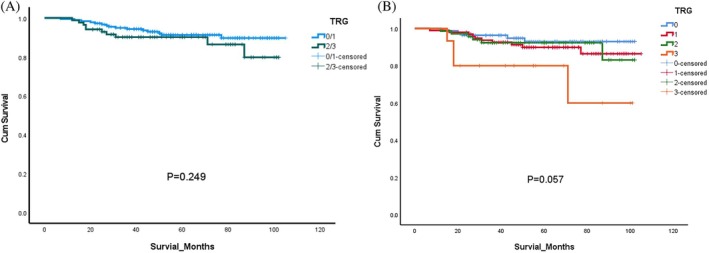
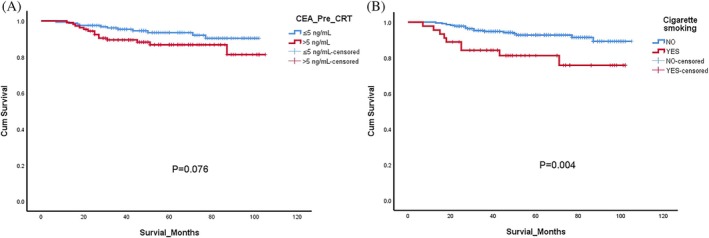
Neoadjuvant chemoradiotherapy (NACRT) is the standard treatment for patients with locally advanced rectal cancer (LARC). Tumor regression grade (TRG) is an essential prognostic factor in determining treatment efficacy. However, the potential factors influencing TRG in patients with rectal cancer who have received NACRT have not been investigated. We conducted a retrospective analysis of patients with LARC who received NACRT followed by surgical resection. We collected data on the patient characteristics, including age, sex, comorbidities, tumor size, lymph node status, time between NACRT and surgery, and pretreatment carcinoembryonic antigen (CEA) levels. TRG was determined on the basis of a pathological assessment of resected specimens, and overall survival (OS) at 5 years was determined. Univariate and multivariate logistic regression models were employed to evaluate the association between the patient characteristics and TRG. Univariate analysis revealed that smoking and prechemoradiotherapy (pre-CRT) and preoperative CEA levels were significantly associated with TRG. In a multivariate analysis, both smoking and higher pre-CRT CEA levels were identified as significant predictors of a high TRG. The hazard ratios were 2.32 (95% confidence interval [CI]: 1.06-5.07, p = 0.036) for smoking and 3.1 (95% CI: 1.69-5.68, p < 0.001) for higher pre-CRT CEA levels. In Kaplan-Meier analysis, the nonsmoker group exhibited higher OS (p = 0.004). Elevated pre-CRT CEA levels and current smoking status were associated with a more than two fold increase in the risk of a higher TRG after NACRT. Moreover, smoking was a significant risk factor for poor OS in patients with LARC following NACRT.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


